
Author: Dave McCreary, Doug West / Codes: RP4, SLO3, SLO4, TP3 / Published: 23/01/2015
In the first of my official LTC podcasts recorded live at the conference I interview Mr Doug West, Consultant Thoracic Surgeon at Bristol Royal Infirmary. During this interview we discuss his talk on surgical fixation of flail chests, finger thoracostomy, and the potential dangers of chest drains – yes, complications happen, and when they do, they can be bad – always proceed with caution!
For those who would like to review the literature yourselves I’ve included references below with links to the NICE guidelines for chest fixation(3) and the references for those(4).
While the concept of rib fixation isn’t new, with initial attempts dating back to the 1950s. There has been a recent move towards formal internal fixation of flail chests that is supported by evidence from several RCTs.
I include below a summary of the review of some of this literature by Leonie Walker, a 5th year medical student who recently completed a placement with the orthopaedic team who are performing rib fixation at Aintree University Hospital in Merseyside.
Tanaka et al 2002(1)
- N = 37 patients with flail chest (> 6 ribs fractured)
- Randomised 5 days post injury
o 18 to surgical stabilisation
o 19 to internal pneumatic stabilisation (positive pressure ventilation to stabilise the rib internally)
- Surgical group had:
o Fewer ICU days (mean 16.5 vs 26.8)
o Fewer mechanical ventilation days (mean 10.8 vs 18.3)
o Lower incidence of pneumonia at 21 days (22% vs 90%)
o Fewer tracheostomies at 21 days (3 vs 15 patients)
o Better return to full time work at 6 months (11/18 vs 1/19)
Granetzny et al. 2005(2)
- N = 40 patients with flail chest (≥3 fractured ribs with paradoxical movement)
- Randomised 24 hours after arrival to ICU
o Group I – Conservative management with strapping and packing for 7-10 days.
o Group II – Surgical fixation within 24-36 hours of ICU admission
- Surgical group had:
o Fewer ICU days (9.6 vs 14.6)
o Fewer mechanical intervention days (2 vs 12)
o Lower incidence of pneumonia (10% vs 50%)
o Reduced hospital length of stay (11.7 vs 23.1 days)
o Lower incidence of chest wall deformity
o Better FVC at two months
There are several other studies used in the formulation of the NICE 2010 Guidance, and they are included by the NICE evidence summary(4).
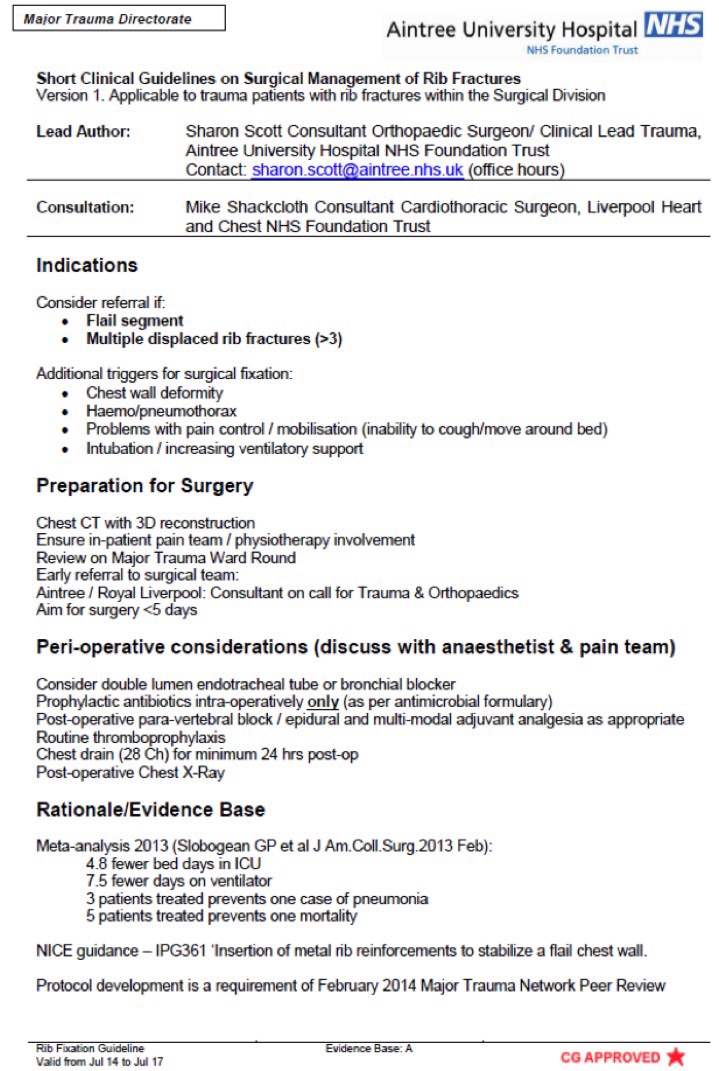
As discussed in the podcast, the MTC at Aintree University Hospital has orthopaedic surgeons performing rib fixation, lead by Sharon Scott, Consultant Orthopaedic Surgeon & Clinical Lead for Trauma. Sharon has kindly provided me with a copy of their clinical guidelines for management of these patients which you can find in the appendix.
Author: David McCreary (@dmccreary85 / @FOAMedNW)
With thanks to: Leonie Walker, 5th Year Medical Student, University of Liverpool & Mrs. Sharon Scott, Consultant Orthopaedic Surgeon & Clinical Lead for Trauma, Aintree University Hospital, Merseyside
References
- Tanaka H, Yukioka T, Yamaguti Y, Shimizu S, Goto H, Matsuda H, et al. Surgical stabilization of internal pneumatic stabilization? A prospective randomized study of management of severe flail chest patients… including commentary by Wilson RF. Journal of Trauma 2002;52(4):727-32.
- Granetzny A, Boseila A, El-Aal MA, Emam E, Shalaby A. Surgical versus conservative treatment of flail chest. Evaluation of the pulmonary status. Interactive Cardiovascular and Thoracic Surgery 2005;4(6):583-7.
- https://www.nice.org.uk/guidance/ipg361/resources/guidance-insertion-of-metal-rib-reinforcements-to-stabilise-a-flail-chest-wall-pdf
- http://www.nice.org.uk/guidance/ipg361/evidence/insertion-of-metal-rib-reinforcements-to-stabilise-a-flail-chest-wall-overview2
Appendix One
Guidelines on Surgical Management of Rib Fractures at Aintree University Hospital

Thoracic Trauma
For each life-threatening thoracic injury this session includes: a definition and context, Clinical assessment , treatment and Key learning points.

Chest Drain Insertion in Adult Trauma
This session provides training in chest drain insertion. It looks at the indications for carrying out this procedure, as well as how to prepare for it, and shows a chest drain being inserted. Post-procedure management and complex cases are also covered

Emergency Care Incubator Members content
Emergency Care Incubator Members content