
Author: Duncan Russell, Shobhan B Thakore / Editor: Gavin Lloyd / Reviewer: Thomas Mac Mahon, Grace McKay / Codes: ACCS LO 1, PC1, PC2, PC3, PC4, RP1, SLO6 / Published: 19/04/2021
The aim of procedural sedation is to relieve a patient’s anxiety towards, and facilitate their cooperation with, a potentially painful procedure, such as a manipulation of a fracture or dislocation.
The general principles of managing painful procedures in ED are:[1]
- Patient explanation, in order to alleviate anxiety
- Identify potentially painful components of the procedure in advance so that local anaesthetic or systemic analgesic drugs can be administered
- Prevent pain whenever possible. Most sedative agents have no significant analgesic effect, therefore analgesia is recommended beforehand.
- Drug sedation should not be used for operator convenience, but as a supplement to behavioural management
- When conscious sedation is employed, the agents and doses chosen must be adjusted to the individual patient
- Formal competency-based training is recommended for all practitioners because these techniques have the potential to cause life-threatening complications particularly in elderly patients or those with co-morbidities.
Definition
Procedural sedation and analgesia should provide pain relief and produce a state of reduced consciousness where the patient is still able to respond to a verbal or physical stimulus and to continuously maintain a patent airway and adequate ventilation.[2]
Basic science
The degree of central nervous system depression achievable using sedative agents ranges from mild anxiolysis to complete loss of consciousness, with marked associated cardiovascular and respiratory depression (figure 1).[2]
If a patient cannot respond to verbal or simple physical stimulation then they require the same level of monitoring and supervision as a patient undergoing general anaesthesia. The practitioner performing the procedure must also have the appropriate level of training and skill.[1]
Dissociative sedation is a separate class of sedation. It is a trance-like cataleptic state, characterised by profound analgesia and amnesia, but with retention of airway reflexes and cardiopulmonary stability. Ketamine is the only agent in sedation practice which achieves this state
The Sedation Continuum
- Alert-anxious
- Alert-calm (anxiolysis)
- Drowsy but clear mentation (sedation)
- Eyes open; speech slurred
- Eyes closed but answers questions appropriately
- Opens eyes to voice; is confused
- Oxygen desaturation on room air
- Opens eyes to pain; responds purposefully
- Eyes closed; moans and withdraws from pain
- Moans to pain. Non-specific motor response to pain
- CO2 retention
- Oxygen desaturation on 2L O2
- No response to pain
- Bradycardia poor gag reflex
- Apnoea hypotension
- Death
When is procedural sedation appropriate?
Indications for procedural sedation
Typically this will be for reduction of a fracture or dislocation [3,4]. Other indications include incision and drainage of an abscess, laceration repair, lumbar puncture, change of burns dressings or cardioversion
Contraindications for procedural sedation
Procedural sedation is contraindicated in the ED when:
- Appropriately trained personnel are not available to perform the sedation.
- Patients have an American Society of Anesthesiologists (ASA) classification of unstable class II or class IV and above (unless requiring immediate intervention, e.g. ventricular tachycardia)
- Appropriate monitoring and resuscitation equipment are not available.
- A general anaesthetic would be more appropriate.
- The patient has an allergy or hypersensitivity to the relevant medications.
- There is a high risk of aspiration e.g. acute alcohol intoxication.
- The patient declines procedural sedation
How can I identify at risk patients?
It is essential that a clinical assessment is made to identify patients who have a high ASA classification or during deeper levels of sedation.[3,4]
| ASA classification | Health status of patient |
| I | A normal healthy patient |
| II | A patient with mild systemic disease |
| III | A patient with severe systemic disease |
| IV | A patient with severe systemic disease that is a constant threat to life |
| V | A moribund patient who is not expected to survive without the operation |
| VI | A declared brain-dead patient whose organs are being removed for donor purposes |
Figure 2: American Society of Anesthesiologists classification system.
It is essential that a clinical assessment is made to identify patients who:
- have a ASA classification of IV or above
- may be difficult to ventilate.
This assessment should include a past medical history, drug history and focussed clinical examination to identify any existing medical illnesses, particularly cardiovascular or respiratory disease and allergy. The presence of any anatomic features that may affect airway management should be noted carefully, see figure 3.[2]
- Dysmorphic or asymmetrical facial features
- A beard
- Significant malnutrition or cachexia with sunken cheeks and missing teeth
- Facial trauma, particularly lacerations through the cheek or unstable bony injuries
- Limited neck extension
- Obesity
- Poor mouth opening of less than 4-5 cm which restricts access
Features that may affect airway management
Sedation of patients with an increased risk of adverse events requires a greater level of experience and training. Consider the urgency of the situation and whether a general anaesthetic delivered in an anaesthetic room is more appropriate.
Fasting
Aspiration is a rare complication of procedural sedation.[3,5]
There is a paucity of evidence to make absolute recommendations regarding minimum fasting times prior to procedural sedation; however the following principles should be borne in mind:
- Protective airway reflexes are more likely to be impaired with deep sedation, making aspiration more likely in the event of regurgitation.
- In circumstances where life or limbare not threatened, a procedure may be delayed to ensure safer sedation without altering the clinical outcome.
Guidelines for fasting for general anaesthesia of 2 hours for clear fluids and 6 hours for everything else should generally be followed
Midazolam
- Midazolam is a fast acting water soluble benzodiazepine that has been used for procedural sedation in the ED for approximately 30 years. It has no analgesic properties.
- Midazolam should be prepared as a 1 mg in 1 ml solution [7].
- The recommended intravenous dose for midazolam is 2-2.5 mg initially, with further 1mg doses repeated after 2-5 minutes, titrated to effect [1].
- The initial dose is 0.5-1 mg in adults older than 60 and the chronically ill or debilitated, with 0.5mg aliquots thereafter.
- Midazolam should be given at a rate of approximately 1 mg over at least 30 seconds; the time to effect is approximately 3 minutes.
- A total dose of more than 5 mg is not usually necessary in a healthy young adult; less than 3.5 mg in adults older than 60 and the chronically ill or debilitated.
- An important safety feature of midazolam is the availability of flumazenil. This rapidly reverses the depressant effects of benzodiazepines. It should not be used routinely, but only in cases of emergency.
- Care must be taken as flumazenil may have a shorter duration of action than the sedative agent, resulting in re-sedation [7].
- The use of flumazenil should be regularly audited as a marker of excessive dosage of midazolam [3].
Propofol
- Propofol is a lipophilic agent that is thought to enhance GABA inhibitory neurotransmission. It is used widely in anaesthesia induction and maintenance [1].
- Propofol is used for procedural sedation in many EDs worldwide [10]. It has a rapid onset and recovery from sedation with complication rates that are comparable with midazolam, making it particularly useful for procedures that require a very brief period of sedation. It is reported to be associated with less apnoea than midazolam, but with slightly more aspirations and intubations [9]; however, formal comparison with other agents used in PSA was inconclusive [11].
- Propofol is associated with profound hypotension and respiratory depression, and frequent induction of deep sedation or general anaesthesia [1].
- Most patients will require 0.5 -1 mg/kg for onset of sedation; further doses of 0.25-0.5mg/kg can be given every 3-5 minutes, titrating to effect.
- 10-20mg boluses given slowly should be used in the elderly and chronically ill or debilitated [1].
- The respiratory depressant effects of midazolam and propofol are enhanced when used in combination with an opiate. When opiate analgesia is required, it should be given first and allowed time to become maximally effective before sedative administration.
- Appropriate training is required prior to its use, following local protocols.
Ketamine
- Ketamine is a dissociative anaesthetic and analgesic that produces a trance-like state due to dissociation between the limbic and cortical systems.
- Patients sedated with ketamine appear to be awake and have little cortical depression, but the awareness of external stimulation is blocked. It is unique in that it produces a state in which respiration and airway reflexes are usually maintained.
- A dose of 1 mg/kg intravenously delivered over at least one minute, or 4-5 mg/kg intramuscularly will rapidly produce a dissociative state lasting up to 30 minutes.
- A reduced dose in the elderly of 10-30mg intravenously is appropriate.
- A problem is emergence phenomena. This may be related to pre-sedation agitation and can be attenuated by minimising stimulation during recovery and avoiding premature awakening.
- Administration of a benzodiazepine, to treat or prevent emergence phenomena is likely to prolong the recovery phase.
- Ketamine is also associated with sympathetic stimulation causing tachycardia and hypertension.
- Ketamine is relatively contraindicated in patients with airway instability or tracheal pathology, a high predisposition to laryngospasm or apnoea, severe cardiovascular disease, CSF obstructive states, previous psychotic illness, hyperthyroidism or thyroid medication use, globe injury or glaucoma and porphyria [1].
Nitrous oxide
- Nitrous oxide has been used as an inhalational analgesic and anaesthetic agent since the 1800s.
- Its analgesic and anxiolytic effect is reliable and dose related and the recovery is rapid once inhalation of the agent ceases.
- It is usually administered from cylinders containing the gas premixed with oxygen at a concentration of 50%, delivered via a demand valve which allows some patient control.
- It is useful as a sole analgesic for minor procedures or as an adjunct to opiate analgesia for moderate to severe pain [12].
- When the inspired concentration of nitrous oxide reaches 70% (the routine anaesthetic dose) consciousness is lost and the same standard of care as general anaesthesia is required [13].
- It is important to be aware of this if a method of delivery other than that described above is used, i.e. an anaesthetic machine. The concentration of oxygen in the inspired gas must never be less than 30%.
Nitrous oxide rapidly diffuses into closed air spaces causing volume expansion and pressure effects. It is contraindicated when there is any suspicion of pneumothorax, bowel obstruction, ruptured viscera or decompression illness (potential air embolism).
Minimum staffing levels for Emergency Department PSA have been defined as follows [4]:
Minimal sedation with Entonox: One Physician or Emergency Nurse Practitioner (ENP)
Moderate sedation/analgesia with intravenous agents: One Physician providing sedation and one Physician or ENP as operator and one nurse (total of 3)
Deep sedation and dissociative sedation using ketamine:
3 practitioners as for moderate sedation. The Physician administering sedation must be accredited with the Royal College of Anaesthetists Initial Assessment of Competence standards.
Environment, equipment, monitoring and documentation
Sedation should take place within a specifically designated area of the department, i.e. a procedure room or the resuscitation room where oxygen, suction, reversal agents and advance life support equipment is immediately available.
Table 1
|
Cardiac monitor |
Laryngeal masks |
|
Pulse oximetry |
10 ml syringe |
|
BP recording set at 5 minute intervals |
Tie |
|
Oxygen applied and delivered prior to procedure |
Gloves |
|
Suction |
Tourniquet |
|
Tilting trolley |
Venflons |
|
Bag, value, mask system ventilation (BVM) – appropriate sized masks |
Syringes – 5 ml, 10 ml |
|
Selection OP/nasopharyngeal (NP) airways |
Flumazenil |
|
ETT – size 7,8,9 cuffed |
Naloxone |
|
Adjuncts – stylet and gum elastic bougie |
Running IV line with 500 ml 0.9% saline |
|
Short and long blade laryngoscopes |
Defibrillator and emergency drug box |
Minimum monitoring requirements during procedural sedation are heart rate, non-invasive blood pressure, respiratory rate and oxygen saturation. The patient’s sedation level should also be recorded using a recognised scale such as the ASA classification of grades of conscious depression. [6]
Table 2
|
Level of sedation ————- Parameter |
Minimal sedation(anxiolysis) |
Moderate sedation(conscious sedation) |
Deep sedation |
General anaesthesia |
|---|---|---|---|---|
| Responsiveness | Normal response to verbal stimulation | Purposeful response to verbal or tactile stimulation | Purposeful response after repeated or painful stimulation | Unrousable even with painful stimulus |
| Airway | Unaffected | No intervention required | Intervention may be required | Intervention often required |
| Spontaneous ventilation | Unaffected | Adequate | Maybe inadequate | Frequently inadequate |
| Cardiovascular function | Unaffected | Usually maintained | Usually maintained | Maybe impaired |
Sedation should take place within a specifically designated area where oxygen, suction, reversal agents and advance life support equipment is immediately available.
Learning Bite
Minimum monitoring requirements during procedural sedation are heart rate, non-invasive blood pressure, respiratory rate, oxygen saturation and continuous waveform capnography
Documentation
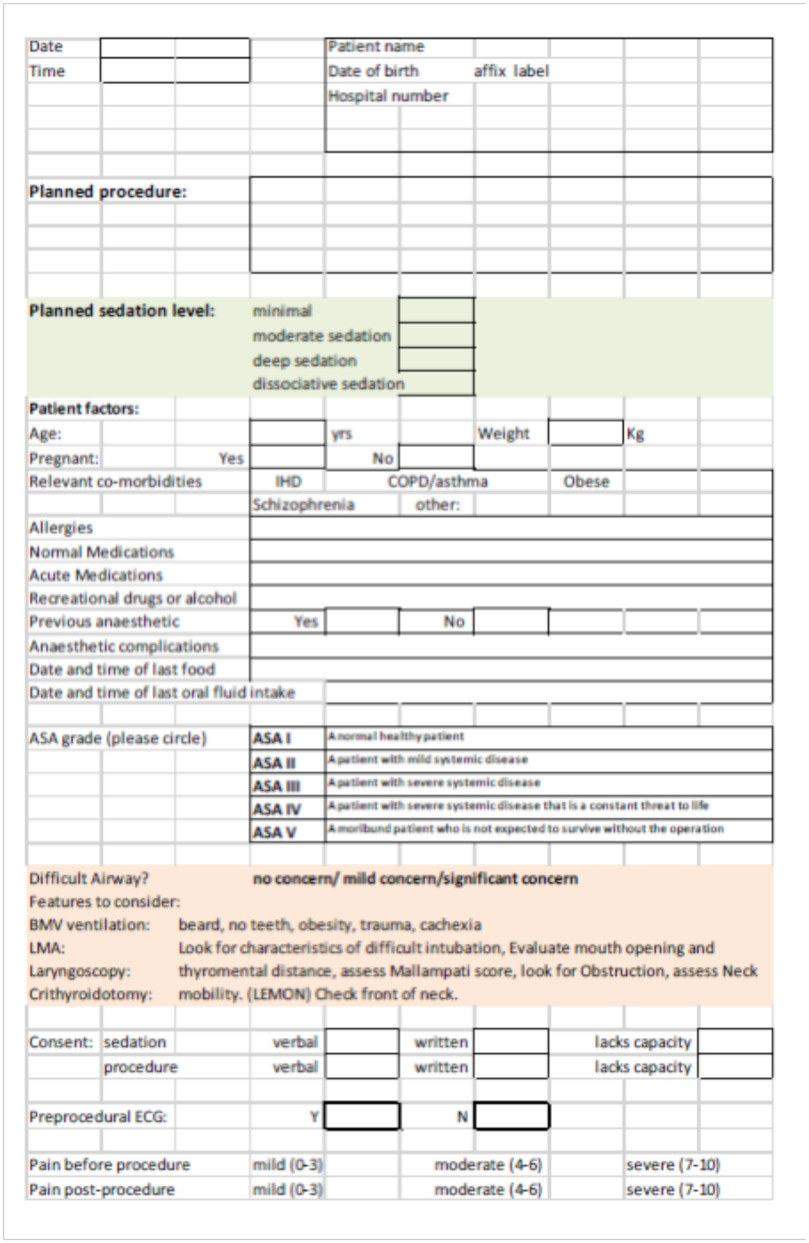
A specific sedation record is recommended for documentation purposes. This should include the patients details, focussed clinical assessment including airway assessment, drugs administered and vital signs during the procedure and until fully alert [1]
Consent
- Valid consent is essential for any procedural sedation and analgesia to be performed [14].
- Information should be provided at an appropriate time (not the last moment), to allow for a discussion and patient questions. Risks and benefits must be clearly explained and a distinction between average and personalised risk made [3].
- Alternatives to sedation (typically general anaesthesia or local anaesthesia with behavioural techniques) should be explained also.
Verbal consent may be sufficient but should be recorded in the patient’s clinical notes
Recovery and discharge
- Removal of the painful stimulus may lead to an increase in the level of sedation during the recovery period.
- This may be accompanied by the development of significant complications and therefore monitoring must be continued until the patient is awake and alert.
- The following serve as reasonable, safe standards for recovery and discharge:
- Recovery should be supervised by trained staff and take place in an area which has adequate levels of monitoring and resuscitation equipment.
- Vital signs should be monitored until the patient is awake and alert, and no longer shows evidence of respiratory depression.
- A physician capable of managing the complications that may arise should be immediately available until discharge criteria have been met.
- Patients should be observed until appropriate discharge criteria are satisfied [3]:
- The patient is alert and orientated, and has returned to their baseline level of consciousness.
- Vital signs are stable and within acceptable limits for that patient.
- Respiratory status is not compromised.
- Pain and discomfort have been addressed.
- Sufficient time must have elapsed since the last administration of any reversal agent (up to 2 hours).
- Patients should be discharged in the presence of a responsible adult who will accompany them home and be able to report any post-procedure complications.
- They should be provided with verbal and written instruction about post-procedure diet, medication, and a phone number to call in the event of an emergency.
Recovery
Discharge:
-
- Post sedation advice form

Airway Assessment







Figure 6: Example of post sedation advice form
Governance
The clinical governance framework for ED sedation should include adequate supervision and training of staff, the use of clinical guidelines and facilities required for safe practice.
The sedation record should be used to facilitate an ongoing audit of the process and outcome of sedation. This should include the incidence of adverse events such as cardiorespiratory depression, over sedation, use of reversal agents, unexpected admission or delayed discharge.
The implementation of these should reduce the incidence of adverse events and improve the quality of procedural sedation, making it safer and a more satisfactory experience for patients and practitioners.
Pitfalls
Pitfalls of procedural sedation are usually a result of inadequate practitioner skills, poor patient selection or a lack of knowledge of the drug being used. When combined, these factors may result in under or oversedation with failure to support a compromised airway, cardiovascular or respiratory system effectively.
Specific pitfalls of procedural sedation include:
- Inadequate provision of analgesia prior to administration of sedative agent.
- Not allowing enough time for the analgesia to reach its maximal effect prior to administering the sedative agent.
- Failure to recognise that the elderly or chronically ill patient requires a lower dose of sedative agent than a healthy young adult.
- Too rapid titration of the sedative agent.
- Not allowing enough time for the sedative to reach its maximal effect prior to attempting the procedure.
- Premature discontinuation of monitoring and transfer of a sedated patient from the safe environment, e.g. from procedure room to x-ray department.
- Discharge with inadequate supervision or written instructions sedative agents cause amnesia and patients may not recall any verbal advice provided.
- The Royal College of Emergency Medicine, Pharmacological Agents for Procedural Sedation and Analgesia in the Emergency Department. Best Practice Guideline. 2016: London, UK.
- Cullinane, M., et al., Scoping our practice. The 2004 report of the National Confidential Enquiry into Patient Outcome and Death. 2004, National Confidential Enquiry into Patient Outcome and Death (NCEPOD): London, UK.
- Academy of Medical Royal Colleges, Safe Sedation Practice for Healthcare Procedures. Standards and Guidance. 2013: London, UK.
- The Royal College of Anaesthetists and The College of Emergency Medicine, Safe Sedation of Adults in the Emergency Department. Report and Recommendations by The Royal College of Anaesthetists and The College of Emergency Medicine Working Party on Sedation, Anaesthesia and Airway Management in the Emergency Department. 2012: London, UK.
- Quality Management and Departmental Administration Committee, Continuum of depth of sedation: definition of general anesthesia and levels of sedation/analgesia. 2014, American Society of Anesthesiologists: Illinois, USA.
- American Society of Anesthesiologists. ASA Physical Status Classification System. 2014 [cited 2016 04 October];
- National Patient Safety Agency Reducing risk of overdose with midazolam injection in adults (NPSA/2008/RRR011). Rapid Response Report, 2008.
- Newstead, B., et al., Propofol for adult procedural sedation in a UK emergency department: safety profile in 1008 cases. Br J Anaesth, 2013. 111(4): p. 651-5.
- Bellolio, M.F., et al., Incidence of Adverse Events in Adults Undergoing Procedural Sedation in the Emergency Department: A Systematic Review and Metaanalysis. Academic Emergency Medicine, 2016. 23(2): p. 119-134.
- Godwin, S.A., et al., Clinical policy: procedural sedation and analgesia in the emergency department. Ann Emerg Med, 2014. 63(2): p. 247-58 e18.
- Wakai, A., et al., The use of propofol for procedural sedation in emergency departments. Cochrane Database Syst Rev, 2015(7): p. CD007399.
- Herres, J., et al., The use of inhaled nitrous oxide for analgesia in adult ED patients: a pilot study. Am J Emerg Med, 2016. 34(2): p. 269-73.
- Myles, P.S., et al., A review of the risks and benefits of nitrous oxide in current anaesthetic practice. Anaesth Intensive Care, 2004. 32(2): p. 165-72.
- General Medical Council. Consent: patients and doctors making decisions together. 2008;

Procedural sedation in Emergency Medicine 2020
Sedation is a routine aspect of emergency care. The aim is clear: make the procedural experience as comfortable as possible for your patient, whilst ensuring that your practice is safe.

Ketamine Sedation in Children
Ketamine sedation is ideal for short, painful or frightening procedures.

Propofol for Procedural Sedation in Adults
This module covers indications for propofol sedation, identifying at risk patients, a standardised procedure, strategies for addressing adverse events, a section on advanced procedural sedation and all the relevant governance issues.
28 Comments
thumbs up
Core knowledge and standards
Good review of essentials.
very useful, thank you
Very useful
really good basics
Covers the basics well
very helpful
Helpful material
Helpful!
comprehensive review
Useful basics for adult procedural sedation. Should keep in mind that appropriate sedation includes analgesia
Very useful
Excellent review, very helpful.
Great learning
thanks
very comprehensive and to the point
A great guidance in sedating patient in ED for a procedure.
very useful
Very rich and informative
Quite useful
Good revision
very helpful n informative
Good Fundamentals and core knowledge.
very useful for PSA in ED
Concise and to the point.
Useful and applicable.
A good reference for pre/intra and post preparation check list.
Very useful especially whilst on Anaesthetic rotation
Concise and to the point.
loved the pitfalls and the discharge criteri.