
Author: Kellie Bateman / Editor: Nigel Poland, Catherine Miller, Chris Wearmouth / Reviewer: Beth Newstead / Codes: / Published: 14/04/2021
Testicular pain is a common presentation to the emergency department. Patients presenting with testicular pain should be rapidly assessed and assumed to have testicular torsion until proven otherwise. Torsion occurs in 1/4000 under 25 year olds, is a surgical emergency and if not assessed and operated on within 6 hours can result in irreversible damage can develop(1). Untreated torsion can lead to testicular ischaemia, infarction, subfertility and the potential need for orchidectomy.
What challenges does scrotal pain present to the emergency physician?
Challenges for the emergency physician can include difficulty in confirming or refuting the diagnosis. It is vital the Emergency physician can appropriately recognise testicular torsion as a potential diagnosis and promptly refer to the acute surgical team for further assessment and management.
Anatomy of the testicle
The average adult testicle is paired and measures 4x3x2.5cm(2).

Figure 1: Anatomy of the testicle(3)
During embryological development, the testis descends from the posterior abdominal wall, through the inguinal canal to the scrotum. The nervous and arterial supply and the venous and lymphatic drainage travel the same route in the spermatic cord. The testis is suspended in the scrotum by the spermatic cord(3).

Figure 2: Bell Clapper Deformity by Todd Buck(17)
The tunica vaginalis is derived from the abdominal peritoneum and separates the testis and epididymis from the scrotal wall. It covers the exterior anterolateral aspect of the testis, fully surrounding the testis and fixing it to the posterior wall. Fluid may accumulate in the tunica vaginalis leading to hydrocele (water), haematocele (blood) or pyocele (pus).
In the bell-clapper deformity, there is high investment of the tunica vaginalis, leading to a horizontal lie and increased free space for the testicle to move within (figure 2). This can then lead to testicular torsion as the spermatic cord twists cutting of the blood supply to the testicle. It is thought approximately 10% of the male population have this deformity, but torsion happens less frequently, with no clear triggering event identified(4).
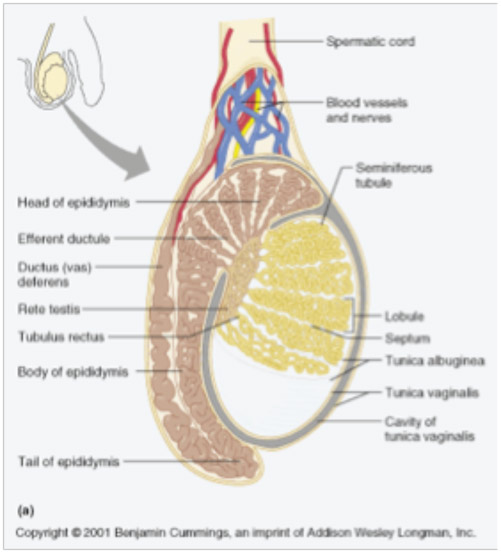
The tunica albuginea is a dense fibrous fascia that encloses the testis. Posteriorly it penetrates the parenchyma of each testis forming the mediastinum and separating each testis into approximately 250 lobules.
The functions of the testes are sperm production and hormone synthesis. Each lobule contains 1-4 convoluted seminiferous tubules The basement membrane of these tubules contain 2 cell types: Sertoli cells, which support the structure and spermatogenic cells which produce sperm. The stroma between the cells contains connective tissue which contains the Leydig cells; these are responsible for producing testosterone in response to luteinising hormone (LH).
Once produced in the seminiferous tubules, the developing spermatozoa collect in the rete testis before travelling via the efferent tubules to the epididymis for storage. The epididymis sits in the postero-lateral aspect of the superior pole of the testes. (3)
The testicular appendages (the appendix testis and appendix epididymis) are embryological remnants that serve no purpose but may twist and cause pain. This is common in pre-pubescent boys and doesnt require surgical intervention if the diagnosis is certain.
Blood Supply to the Testes
The arterial supply to the testes derives directly from the aorta where the gonadal arteries branch off at L2, just below the renal arteries. The testicular arteries travel in the spermatic cord with the cremasteric and differential artery, where they anastomose with the vasa deferentia that branch off the internal iliac artery.
Blood from the testes drain into a network of veins within the scrotum called the pampiniform plexus. This allows counter current cooling of the testis to maintain function. Defective valves or compression of the veins can cause them to become enlarged leading to varicoceles. Varicoceles can sometimes cause an aching or dragging sensation within the scrotum. At the junction of the internal inguinal ring the pampiniform plexus becomes the spermatic vein. The right spermatic vein then drains directly into the vena cava, just below the renal vein. The left spermatic vein drains into the left renal vein before it joins the vena cava, this differing pathology means that a left renal cancer may present with a left sided varicocele and these should always be investigated

Learning Bite
Testicular torsion is due to the spermatic cord twisting, leading to ischaemia of the testis and requires emergency surgery. Torsion of the testicular appendages is a benign condition requiring supportive treatment.
Nervous Supply to the Testes
There is extensive nervous supply to the testis and scrotum and pain felt in the scrotum may be referred from visceral or somatic structures.
The autonomic nerve supply of testis is supplied by the testicular plexus which orginates from the paraaortic ganglia. Ramus genitalis (a branch from the genitofemoral nerve) and the Ilioinguinal nerve supply the scrotal skin and muscles in the groin area.
Learning Bite
Conditions affecting the scrotum can cause referred pain to the abdomen. Conversely, pathology within the abdomen may cause referred pain to the scrotum. Males presenting with abdominal pain should always have their scrotum examined and vice versa.
Lymphatic drainage
Lymphatic drainage from the testes drains to the lumbar and para-aortic nodes at L1. Therefore, testicular cancers or infections (orchitis) may not lead to palpable lymphadenopathy. This also affects the surgical approach for testicular cancer with surgery taking place via the groin rather than taking a scrotal approach.
Lymphatic drainage from the scrotum drains to the superficial inguinal nodes.
Primarily, it is most important to distinguish if the presenting complaint is actually acute testicular pain (which is potentially a surgical emergency) or scrotal swelling (which should be relatively painless)
The most common cause of acute testicular pain are:
Testicular Torsion
Definition: Twisting of the spermatic cord, cutting of the blood supply to the testicle, leading to ischaemia(5). This requires urgent detorsion and fixation (orchiopexy) before the testicle becomes ischaemic and needs removal (orchidectomy). Ideally surgery should be performed within 6 hours before the testis becomes unsalvageable(6)
Epididymo-orchitis
Definition: Inflammation of the epididymis +/- testes, leading to acute pain or swelling. It may be caused by a sexually transmitted infection or other urinary tract infection spreading along the urinary tract and should improve with antibiotics (7).
Torted appendages
Definition: Twisting of the vestigial appendages of the testis or epididymis. This can lead to pain and may mimic testicular torsion but does not cause damage to the testis and can be managed conservatively.
Learning Bite
Testicular Torsion is an acute surgical emergency and must be confidently excluded before other diagnoses can be considered
Other causes of acute testicular pain include:
- Trauma
- Inguinal Hernias
- Forniers Gangrene
- Malignancy
- Oedema/Swelling
- Cysts/Hydroceles
- Referred Pain e.g. Renal Colic, AAA
History
The three most important details to obtain are the patient’s age, the description of the pain and a sexual history(8). No single factor in the history can reliably distinguish torsion.
Age
As shown in table 1, different age groups make certain diagnoses more likely. Testicular Torsion has a bi-modal distribution typically presenting in neonates and post puberty. Appendiceal torsion is more common in pre-pubertal boys.
Table 1: The age distribution for common causes of acute scrotal pain found at exploration. Adapted(9)
| Age (years) | Testicular Torsion | Appendix Torsion | Epididymitis | Normal |
| 0-11 | 6.6% | 62% | 6% | 25.4% |
| 12-16 | 52% | 32% | 3% | 13% |
| 17-40 | 48% | 5% | 27% | 20% |
Learning Bite
Testicular Torsion can present at any age but is less common in the elderly.
Pain History
A thorough pain history can establish if the pain is true acute onset testicular pain fitting with testicular torsion or is referred from other pathology. Acute onset of pain is typically associated with testicular torsion with one study recently finding sudden onset of pain was seen in 90% of patients with testicular torsion, in 69% of patients with appendix torsion, in 58% of patients with epididymitis, and in 78% of patients with normal scrotums(10).
Gradual onset pain is classically more likely to be torsion of the appendage, but may also correlate with a history of intermittent torsion.
Previous torsion and orchidopexy (which is typically done bilaterally) makes further torsion highly unlikely.
Sexual History
Sexually transmitted infections are a common cause of epididymo-orchitis. Eliciting a sexual history can help guide treatment by revealing risk factors such as: previous sexually transmitted infection, urethral discharge, number of sexual partners in the past 12 months, men who have sex with men. Men who perform penetrative anal intercourse are also at risk of infection with enteric organisms due to exposure to gastrointestinal flora(7).
Other aspects of the history
Testicular torsion typically presents in a post-pubertal male with sudden onset severe, unilateral, testicular pain. There may be a history of similar episodes of self limiting pain indicating spontaneous torsion and detorsion (intermittent torsion). Precipitants may be related to forceful contraction of the cremasteric muscle secondary to trauma, physical exertion, an erection or sudden coldness. Associated features include: anorexia, gastrointestinal upset and fevers(11).
Other causes of epididymo-orchitis to be aware of include mumps (fevers and parotid gland swelling) and vasculitides such as Buergers syndrome and Henoch-Schnlein purpura (rash and arthralgia).
The patients past medical history may reveal other differentials such as: hernias, renal stones, aortic abdominal aneurysm.
Examination should respect the patients privacy and assess the abdomen, scrotum and penis. Consent should be gained and a chaperone should be present.
The abdomen: Assess for tenderness, hernias and lymphadenopathy
The scrotum and penis
Inspection: Look for swelling, erythema, the lie of the testicle, penile rash/dishcharge. The Blue Dot Sign may be difficult to see but occurs in a torted testicular appendange (12)
Palpation: Palpate the testicle and scrotum to assess any masses or tenderness. Localised oedema may develop rapidly in torsion making assessment difficult.
Is it within or surrounding the testis? Typically, in epididymitis the pain is localised there, as opposed to torsion where the pain is diffuse.
How does the testis lie? The normal testis rests vertically with the epididymis above the superior pole in a posterolateral position. A torted testis is often high riding with a horizontal lie.
Special Tests: The Cremasteric Reflex is elicted by stroking the inner thigh, and elevation of the ipsilateral testis should be observed if present. In testicular torsion this reflex is commonly absent with a high (but not absolute) negative predictive value(13). Prehns Sign is demonstrated by elevating the scrotum which in theory relieves the pain of epididymitis, but not torsion.
Learning Bite
History and Examination may make one diagnosis more likely than another, but no key feature can completely rule out torsion.
Differentials
| Trauma | Testicular trauma may cause torsion, testicular rupture or haematoma which should be referred to a urologist or surgeon for a specialist opinion and possible intervention. |
| Inguinal Hernias | May have a history of fluctuant testicular swelling. These have the potential to become irreducible and incarcerated causing pain and discomfort. |
| Fourniers Gangrene | This is necrotising fasciitis of the perineum and is a urological emergency. It is more common in diabetes and vasculopaths. Presents with severe pain and rapidly spreading necrotic cellulitis. |
| Malignancy | Testicular cancers typically present in men aged 15-40 years with a small hard lump within the testis with/without pain. If any concern an USS may be indicated. |
| Oedema | Peripheral oedema may progress up the legs to the testes causing diffuse swelling and pain; this will require diuretics and medical management. |
| Cysts/Hydroceles | Cyst and hydroceles should be relatively painless, but may cause a heavy or dragging sensation. |
| Referred Pain e.g. Renal Colic, AAA, Appendicitis | Abdominal pain may be referred into the groin and testes. It is important to complete a thorough abdominal examination and consider these differentials, particularly in older patients. |
Some risk stratification tools have been developed, particularly for paediatric cases where history is unreliable. However, due to implications of a missed testicular torsion these have not been verified and used independently.
Laboratory Evaluation
Blood results are of little importance as they take time to process and may show a raised White Cell Count (WCC) in both torsion and epididymitis
Urinalysis may indicate an underlying urinary tract infection but may not confirm or refute either diagnosis.
Screening and swabs for sexually transmitted infections may be necessary to guide treatment if epididymitis is suspected from the history (7) The results of such tests will clearly not be available for use in the ED.
Radiologic Imaging
Imaging tests include: Doppler ultrasonography and nuclear scintigraphy, but their use is still highly controversial, with delays for imaging being termed as castration through procrastination(14).
Doppler ultrasonography is thought to be useful in equivocal cases with a high sensitivity for confirming increased blood flow seen in epididymitis, but in small children it often detects no blood flow in normal testicles(15).
Nuclear scintigraphy detects the accumulation of IV technetium in the testis. In torsion there is no technetium seen in the testicle. The major downfall of this test is that it takes time (20-30minutes) and isnt always available.
In the U.K. imaging is only indicated in late presenters with an unclear diagnosis under senior review.
Learning Bite
Surgical exploration for suspected testicular torsion should NEVER be delayed for imaging.
As previously discussed, if testicular torsion is suspected, the testicle must be explored to confirm or refute the diagnosis.
Testicular Torsion
Treatment for suspected testicular torsion is immediate surgical exploration with intraoperative detorsion and fixation of the testes. Studies have found that testicular tissue becomes increasingly unsalvageable from 4-6 hours. Reported testicular salvage rates are 90% to 100% if surgical exploration is performed within six hours of symptom onset, decrease to 50% if symptoms are present for more than 12 hours, and are typically less than 10% if symptom duration is 24 hours or more(16). Even if the diagnosis has been delayed the scrotum should still be explored. If the testis is ischaemic and unsalvageable an orchidectomy may be indicated to prevent formation of anti-sperm antibodies leading to infertility. Patients should ideally have pre-operative counselling regarding this.
Whilst awaiting surgery it is important to manage symptoms with analgesia and antiemetics. Manual detorsion may also be attempted as an adjunct to surgery. This is typically done by rotating the testicle from medial to lateral (clockwise) and usually require at least 360 degrees. This is only a temporary measure whilst awaiting surgery and requires strong analgesia +/- sedation +/- nerve blocks. (16)
Torsion of the appendages
Torsion of the appendages cause no damage to the testis and can be managed conservatively with NSAIDs, ice and support. Pain typically lasts a week and is self-limiting. It is important to reassure parents. This is clearly a diagnosis of exclusion.
Treatment for epididymitis depends on the likely pathogens responsible and testicular torsion must be confidently excluded prior to treatment. National guidelines developed by British Association for Sexual Health and HIV (BASHH) recommend(7):
- Having a very low threshold for excluding testicular torsion
- Rest, analgesia (NSAIDs if appropriate) and scrotal support
- Empirical antibiotic treatment based on initial assessment prior to culture results
- If antibiotics are started in ED, a first pass urine should be sent for C. trachomatis and N. Gonorrhoea, as well as a urine dip/mid-stream urine MC&S.
- All patients with probable STI should be advised to abstain from sexual intercourse and attend an appropriate sexual health (GUM) clinic for STI testing.
If Sexually-Transmitted infection suspected treatment is typically (young patient, new or multiple sexual partners, lack of consistent condom use, known STI contact):
Ceftriaxone 1g IM single dose, PLUS doxycycline 100mg PO BD for 10-14 days
If an enteric pathogen is likely (older patient, not sexually active, recent instrumentation, urine dipstick positive for leukocytes and nitrites):
Ofloxacin 200mg PO BD for 14 days, OR
Levofloxacin 500mg PO OD for 10 days, OR
Co-amoxiclav 625mg PO TDS for 10 days
Click here for 2019 BASHH guidelines.
If Mumps suspected, antibiotics are not indicated and should be treated as per Mumps: NICE Clinical Knowledge Summary.
Patients with epididymo-orchitis typically can be discharged home and do not require hospital admission unless they are: struggling to manage symptoms; particularly unwell (septic); immunocompromised.
It is important to safety-net patients discharged home. Advise the patient symptoms should begin to improve within 3 days of starting treatment but may persist for up to 6 weeks. If there is persistence of symptoms patients may require a testicular ultrasound +/- specialist urological or sexual health follow-up to ensure the appropriate treatment was given, that an abscess hasn’t developed and that there isn’t an underlying malignancy.
- Failure to recognise and treat testicular torsion in a timely manner can lead to irreversible damage.
- Failure to acknowledge that the presence or absence of a particular clinical feature still cannot exclude torsion.
- Failure to give prolonged courses of antibiotics in epididymo-orchitis can lead to incomplete treatment and lack of resolution.
- Failure to instigate correct microbiological investigations prior to antimicrobial therapy or to organise appropriate follow up (contact tracing) may result in delayed effective treatment.
- Ringdahl E, Teague L. Testicular torsion. Am Fam Physician. 2006;74(10):173943.
- Manski D. Testis, Epididymis and Spermatic Cord: Gross Anatomy [Internet]. 2016 [cited 2016 Nov 10].
- Teach me anatomy. Testes and Epididymis [Internet]. 2015 [cited 2016 Nov 10].
- Caesar R, Kaplan G. Incidence of bell-clapper deformity in an autopsy series. Urology. 1994;44:114.
- Ogunyemi I. Testicular Torsion [Internet]. Medscape. 2016 [cited 2016 Nov 2].
- Yin S, Trainor JL. Diagnosis and management of testicular torsion, torsion of the appendix testis, and epididymitis. Clin Pediatr Emerg Med. 2009;10(1):3844.
- British Association for Sexual Health and HIV. United Kingdom BASHH national guideline for the management of epididymo-orchitis, 2019. BASHH.
- David JE, Yale S, Goldman IL. Urology: Scrotal Pain. Clin Med Res. 2003;1(2):15960.
- Watkin NA, Reiger NA MC. Is the conservative management of the acute scrotum justified on clinical grounds? Br J Urol. 1996;78:6237.
- Van Glabeke E, Khairouni A, Larroquet M et al. Acute scrotal pain in children: Results of 543 surgical explorations. Pediatr Surg Int. 1999;15:3537.
- Knight P, Vassy L. The diagnosis and treatment of the acute scrotum in children and adolescents. Ann Surg. 1984;200:664.
- Dresner M. Torsed appendage: Diagnosis and management: blue dot sign. Urology. 1973;1:63.
- Rabinowitz R. The importance of the cremasteric reflex in acute scrotal swelling in children. J Urol. 1984;132:89.
- Lindsey D, Stanisic T. Diagnosis and management of testicular torsion: pitfalls and perils. J Emerg Med 1988;6(1)42-46. 1988;6(1):426.
- Kass E, Stone K, Cacciarelli A et al. Do all children with acute scrotum require exploration? J Urol. 1993;150:6679.
- Sharp V, Arlen A. Testicular Torsion: Diagnosis, Evaluation, and Management. Am Fam Physician. 2013;88(12):83540.
- Buck T. Tunica Vaginalis, Bell – Calpper Deformity and Testicular Torsion [Internet]. 2012.
- Radiologykey. Duplex Ultrasound Evaluation of the Male Genitalia [Internet]. [cited 2016 Nov 26].
Additional Resources:

Male Urological issues in the ED
Urology presentations are fairly common to the emergency department, and we hope this just in time reminder will emphasise some of the key management points.

Testicular Pain
An introduction to the assessment and management of acute testicular pain with reference to the anatomy. This session focuses on the importance of recognising and promptly managing testicular torsion

Let’s twist again…the acute scrotum and torsion
This session is about the assessment and management of patients presenting with testicular pain to the emergency department
11 Comments
great information. very useful
Excellent learning session, very informative and useful in clinical practice.
Very nice resource. Covers everything an Emergency physician needs to know.
A full comprehensive review
good run through acute testicular pain
Good comprehensive information
A very well written resource. Good learning article.
Good overview.
Great document to refresh my memory
very useful review – thank you
Helpful learning session – thank you