
Author: Charlotte Davies / Editor: Liz Herrieven / Codes: SLO9 / Published: 28/05/2019
Immersive manikin simulation is a popular teaching modality in healthcare, with lots of tips everywhere. It’s so popular RCEM does have a simulation committee, and regional leads have been appointed. We thought a brief overview about simulation considerations would help beginners to set out. Much time is devoted to writing the “right” scenario. At our institution it was felt that the amount of time spent writing the scenario was not always proportional to the success of the scenario. There is much literature validating the use of simulation in a wide variety of clinical settings, with many suggestions as to the way each scenario had been run. Here, we look at the existing literature about how to write a simulation scenario, and share some of our tips for success.
1. Check modality?
Immersive simulation is great for situated learning and applying existing skills. It is not a useful modality for teaching new skills, or gaining skill mastery. It is useful at integrating all skills into a realistic environment. Well designed simulation training can contribute to stress inoculation training.
Simulation requires equipment, and a high faculty to learner ratio. Whilst you may think simulation is the ideal training modality, you may not have the resources, including faculty, available to you – and this must be considered.
2. Identify your learners
Think about whether your course is going to be open to the whole multidisciplinary team, or just a single healthcare group. If you are writing scenarios for the entire MDT, there must be roles for everyone – if the only thing your Nurses can do is to take baseline observations or call the Doctor, they will not feel engaged with the process, and the scenario will not be realistic. Having Nurses or other MDT members in the simulation often adds a greater richness to the debrief.
The level of the group must also be taken into account. The learning around a sepsis scenario for an FY1 is very different to that of an ST6.
If you are writing scenarios for juniors and seniors, think about how you will manage that interaction – do you want the junior to hand over to the senior, or do you want them to work together, and display teamwork? You can find scenarios already online (emsimcases, em3, Oxford,)- but check they have the right aim, context and objectives etc.
3. Outcomes and Aim
This is a very broad look at why you are running this scenario. It might be that you’ve set the scenario up in response to an adverse incident, or just because it is a topic that interests you. There should be an intended learning outcome e.g. manage an acute asthma attack and demonstrate an ability to prioritise. Often it works well to have one clinical objective e.g. manage anaphylaxis, with one human factors objective e.g. placate an angry relative. Try to limit the amount of learning objectives, to ensure you have time to cover everything in your debrief.
When thinking of your aim, make sure you include both knowledge and behaviours that you wish to address.
4. Add context and location
You need to make sure you add some authenticity to your scenario to enable you to capture the imagination of your learner. Write down any clinical content – if you base your scenario on a real clinical situation you have encountered, there will be much more authenticity and the learners will notice. Add in features and props to make the scenario realistic. Think about all the sensory modalities. Do you need background noise to make it sound realistic? What props do you need to make it look realistic? What smells do you need? What textures do you need to find?
5. Write objectives
These, like any objectives, need to be SMART. Make sure they cover the main categories of clinical, human factors and management, as dictated by your session aim. Do not try to cover too much in your learning objectives – 3 – 4 in each domain is more than enough.
6. Create flow
Decide how long you would like your scenario to aim for. We normally run for 10 – 15 minutes. Make sure you have a beginning, middle and an end to your scenario:
Beginning – This is your scene setting. You need to think about how you want to introduce this.
Middle – You need to have a change after a trigger action – this is the core challenge of your sim scenario. You need to make sure you embed suitable clues in the scenarios to make sure the right action happens, and these can be subtle or obvious depending on your learner group. A trigger might be a patient saying “I’m really itchy” which may trigger treating anaphylaxis. Observations are useful if you will pre-program your scenario, or if you don’t have clinical input in your control room, but most of the time the simulation technician can change them quickly.
Ending – Attempt to anticipate the ending of your scenario, and think of some alternative endings. Your learning objectives will help with this – you might want to stop an anaphylaxis scenario after the second dose of adrenaline has been given, or you might want to wait a bit longer. It is impossible to anticipate all alternative endings.
Some find it easier to write this scenario progression as a flow chart.
7. Add details
You need to add contextual details to add realism to the scenario. Experienced simulation faculty may be able to “make this up on the day”, but to ensure adequate realism, planning this in advance is advised.
Collate all the information you have so far, and write a scenario overview, list of props, and any notes needed.
8. Add complexity
The basic scenario is likely to run very well, but think about how you will add complexity to the scenario. This might be complexity that happens every time you run the scenario, or complexity that can be added in or not depending on how the learners are doing. It might be that if they’re doing well, you throw in an angry relative, or a drug error – but stick to your learning aim and objectives.
9. Review
Mentally run through the scenario and check it works. Get your fellow faculty members to read the scenario, and see if they think it will work or not.
10. Debriefing and Evaluate
Choose your debriefing model- there are lots of different models that are aimed at different aspects of the scenario. Think how your scenario fits in with the rest of the day – if you have five scenarios that all look at teamworking, your students are going to get very bored! I’m most used to using the debrief diamond which is great for debriefing human factors, but it is rubbish for technical skills. The tables below talk about some different debriefing models, and how which you use will depend on what your debriefing focus is, and your preferred method. Which ever method you use, don’t be afraid to re-inforce good practice.


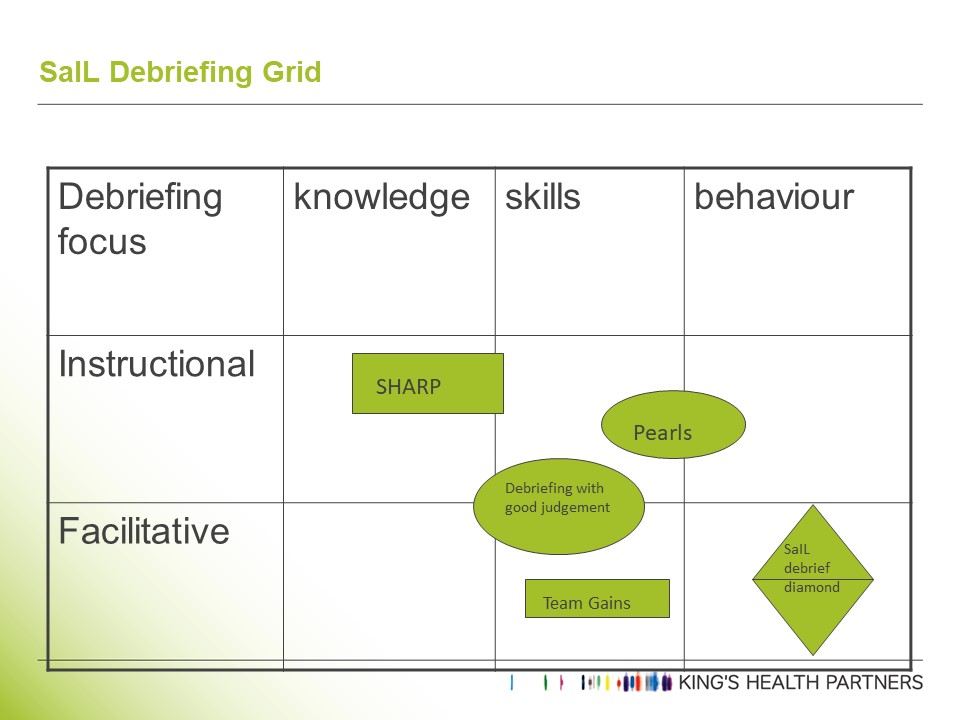
(Image reproduced with permission from Dr Reedy, Kings College London)
If short of time in debrief, ask the students to set the agenda – “what should we cover in 15 minutes?”. Use signposts to branch out – I have a review article on XYZ I will email out – let’s now move on and talk about…
Whichever method you use, before the first debrief set expectations and say why you’ve chosen the model – it helps. Allocate a faculty member to help keep timing – otherwise it’s easy to waffle on. It’s good practice to go very meta, and to “debrief the debrief”. “OSAD” is a tool to help when done formally, and DASH is a great tool for promoting reflection. Focus areas might involve looking at the energy of the group, any poor debrief practice, any good practice. You might want to comment on whether contributions from the entire MDT were acknowledged in an open, curious, enquiring and non-judgemental tone, with the debriefer talking just enough and not too much.
Evaluation of the entire day, after you’ve run it, is the next important part of the day. Our local sim network encourages this, and has a form prompting reflection on specific debrief elements.
Which ever model you use, you’ll need to know something about some of the non-clinical, or non-technical topics you mention. These are the human factor elements. We’ve got blogposts already on stress, time management, situational awareness, decision making, prioritisation, and the emj has some thoughts on distraction . What else would you like us to write about?
There’s lots of further resources you can visit – have a look at EM sim cases for a start.

SLO6 - Practical Procedures
We thought we'd create this mini summary of the resources we've found here and elsewhere to enable you to get the background to proficiently deliver and teach emergency medicine skills.

In-situ simulation: A beginner’s guide
In-situ simulation: A beginner’s guide

A Brief(ish) Guide to Blogging for RCEMLearning
Potential bloggers have frequently asked the RCEMLearning team for a template or some kind of formal guidance about how to write blogs