
Authors: Gary L A Cumberbatch / Editor: Jason M Kendall, Philip Delbridge / Reviewer: Iolo Roberts, Michael Perry / Code: CC5, CC7, CP1, CP4, RP3, RP7, SLO1, SLO3, SLO6, VC2 / Published: 15/12/2023
Context
The challenge for the Emergency Physician is in making the diagnosis of acute aortic dissection and in doing so as expediently as possible as the mortality rate is 1-2% per hour. It is often a difficult diagnosis to make due to the multitude of different clinical presentations of the disease. The aim of this review is to provide a firm knowledge base about aortic dissection and to increase its consideration in the differential diagnosis of any patient with appropriate signs and symptoms of the disease.

The image illustrates an aortic dissection from the ascending aorta into the descending aorta.
Definition
Aortic dissection occurs following a tear in the aortic intima with subsequent separation of the tissue within the weakened media by the propagation of blood.
At the point of dissection the aorta is NOT aneurysmal and the term dissecting aneurysm is incorrect and may be misleading.
A ruptured or leaking abdominal aneurysm is a different disease, requires immediate surgery with only occasional need for any imaging, can be performed in most hospitals by a vascular surgeon and does not require the use of cardiopulmonary bypass.
Classification
Stanford classification
There are 4 different classifications of aortic dissection and the commonest one used is the Stanford classification dividing them into Type A and Type B. A type A dissection involves the ascending aorta and/or the arch whilst type B dissections involve only the descending aorta and occur distal to the origin of the left subclavian artery.
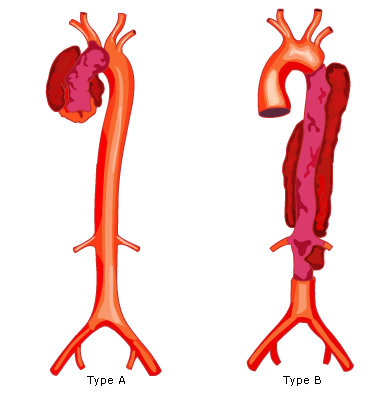
DeBakeys Classification
The other commonly used classification is DeBakeys classification which divides aortic dissections into 3 types: I, II and III (Figure 1). Type I dissections involve the entire aorta whilst type II only involves the ascending aorta and, or the arch of the aorta. Type III involves only the descending aorta.

Figure 1: Classification of aortic dissection: Stanford Classification (Type A and B) and DeBakeys Classification (I, II and III)
Reul and Cooley further subdivided De Bakeys classification into subtypes IIIa and IIIb. In IIIa the dissection involves the aorta just distal to the left subclavian artery but extends proximal or distal to this but is largely above the diaphragm. In IIIb the dissection occurs only distal to the left subclavian artery and may extend below the diaphragm.
Svenssons classification
A more recent classification has been made by Svensson, because intramural haematoma and aortic ulcers may be the only signs of evolving aortic dissection and are not accounted for in the other classification systems.
| Class 1 | Classic dissection with flap between true and false aneurysm and clot in false lumen |
| Class 2 | Intramural hematoma |
| Class 3 | Limited intimal tear with eccentric bulge at tear site |
| Class 4 | Penetrating atherosclerotic ulcer with surrounding hematoma, usually subadventitial |
| Class 5 | Iatrogenic or traumatic dissection illustrated by coronary catheter causing dissection |

Pathophysiology
Aortic dissection occurs following a tear in the intimal layer of the aorta with subsequent anterograde or retrograde flow of blood within the outer third of the tunica media. It is thought that this occurs because of medial degeneration and certain conditions predispose to this (see Table 1).
Table 1: Predisposing factors for aortic dissection
|
Hypertension
|
| Marfans Syndrome |
| Ehlers-Danlos Syndrome |
| Annuloaortic ectasia and familial aortic dissection |
| Bicuspid aortic valve |
| Coarctation of the aorta |
| Pregnancy |
| Turners Syndrome |
| Cocaine abuse |
| Giant cell arteritis |
|
Iatrogenic
|
Notably essential hypertension is by far the commonest risk factor being present in approximately 70% of cases. It causes weakening of the tunica media layer of the aorta.
Marfans Syndrome is associated with an inherited connective tissue disorder resulting in a weakened aortic media and progressive aortic dilatation. Marfans Syndrome is likely to be present in 50% of cases of dissection presenting under the age of 40.
Bicuspid aortic valve is associated with aortic root dilatation and with a congenitally weakened aortic wall.
Intimal tear
The channel created by the dissection process is called the false lumen and occasionally the blood may re-enter the true lumen through a more distal tear in the intima.
The majority of intimal tears occur in the ascending aorta (see Figure 1) due to greater pressure on the aortic wall as it is closer to the left ventricular outflow.

Dissection
Once the dissection process occurs blood tracks through the media to varying degrees and may dissect down from the aortic root to the bifurcation of the common iliac arteries in a matter of seconds and typically causes maximum pain at this time.

aortic dissection from the ascending aorta extending to the bifurcation of the common iliacs.
The incidence of the location of primary aortic tears
| Location of primary aortic tear | Incidence |
| Ascending aorta | 70% |
| Descending thoracic aorta | 15-20% |
| Arch of the aorta | 10% |
| Abdominal aorta | <5% |
Pathophysiological consequences of AAD
1) Rupture into various body cavities (see Table 2):
AAD can result in rupture of the dissection into various body cavities (see Table 2).
| Ascending aorta |
|
| Arch of aorta |
|
| Descending aorta |
|
| Abdominal aorta |
|
(2) Occlusion of any of the branch vessels of the aorta with consequent distal organ ischaemia (see Table 3):
Pulse deficits are a classic feature of AAD and represent occlusion of branch vessels of the aorta. There are two ways this can happen:
- Smaller branches may be simply compressed at the point of origin without the dissection progressing within the tunica media.
- The dissection progresses within the media of the branch vessel and the false lumen becomes so large it compresses the true lumen of the vessel.
Occasionally an obstructed branch vessel can have its blood flow restored either because of a re-entry tear into the true lumen or because an intimal flap only intermittently obstructs the origin of the vessel as the flap extends or moves with aortic blood flow.
Table 4: Branch vessel occlusion and consequences
| Coronary vessel(s) | ST elevation myocardial infarction |
| Common carotid(s) | any type of stroke |
| Subclavian(s) | an acutely ischaemic upper limb |
| Coeliac/mesenteric vessel(s) | ischaemic bowel |
| Renal vessel(s) | frank haematuria |
| Spinal artery(ies) | sudden onset painless paraplegia |
(3) Acute or progressive aortic regurgitation:
This occurs when the dissection process extends into or around the aortic valvular support. When this happens the aortic root can dilate so much that the aortic leaflets cannot fully appose during diastole thereby allowing regurgitation of blood through the cusps. The resultant murmur may be of any grade of intensity and may be inaudible if there is associated haemopericardium. Patients who survive the dissection process may have a delayed presentation with cardiac failure.
A substantial amount of what we now know about the disease is due to the ongoing data submitted to the International Registry of acute Aortic Dissection (IRAD) [1].
The history
The history is the most essential part of the assessment of a patient as it will be the patients symptoms that will alert you to the possibility of aortic dissection. The most common symptom is pain and in 85% of patients in the IRAD series this pain was abrupt in onset. The pain is often so sudden that the patient can describe exactly what they were doing at the moment of onset and the pain is almost always at its maximum at this point. This history helps distinguish between the pain of aortic dissection from the more gradual onset of chest pain that occurs with acute coronary syndromes. In addition the pain of aortic dissection is commonly sharp in nature whilst it is described as an ache or tightness in acute coronary syndrome. The classic tearing interscapular pain was found to occur in only 50% of patients in the IRAD series regardless of whether they had a type A or type B dissection.
The pain in aortic dissection occurs in the anterior chest 70-80% of the time in patients with a type A dissection and back pain occurs only in 50% of all patients [1]. Abdominal pain was found to be the third commonest site of initial pain and other sites described were the throat, neck and extremities.
Patients may also describe the classic migration of pain from the chest, back or abdomen to one or more limbs or to the neck and this is thought to be due to peripheral extension of the dissection from the primary intimal tear. The physician must beware that the pain, however severe initially, may completely resolve by the time the patient presents to hospital and often this is because the dissection process has for the moment stopped or there is relief of the pressure within the aortic wall by the spontaneous re-entry of blood back into the true lumen.
It is on these features alone that the physician should suspect aortic dissection even if subsequent clinical examination and other bedside tests do not support the diagnosis. This suspicion should be raised further if the patient has any of the predisposing factors such as hypertension, Marfans Syndrome, etc.
In 5-15% of patients however, no pain occurs at all and this is typically the case in those patients presenting with syncope, stroke, congestive cardiac failure or the elderly.
Physical examination
The physical examination of these patients needs to be thorough but also must be done quickly. The chest should be specifically examined for a pleural effusion which may represent a haemothorax. A neurological assessment should be carried out since patients can present with stroke, with upper limb weakness, or even with spinal cord infarction.
When examining the cardiovascular system one must search for the following:
- Signs relating to haemopericardium: pulsus paradoxus, faint or absent heart sounds, distended neck veins, shock
- Signs relating to aortic root dilatation: wide pulse pressure, diastolic murmur over the aortic area
- Compression of the true aortic lumen: systolic murmur over any part of the aorta
- Pulse deficits: a difference of 20mmHg or more in blood pressure between arms, a weaker central or peripheral pulse compared to the contralateral side or palpable thrills or audible bruits over pulses
- If the patient is hypotensive one must quickly determine whether this is secondary to hypovolaemia, pump failure or neurogenic as the treatments for each of these is very different.
Hypovolaemia may be caused by a massive haemothorax, loss of blood into an extensive aortic wall false lumen, bowel ischaemia with or without haematemesis or retroperitoneal haemorrhage.
Cardiac failure can be secondary to haemopericardium with tamponade; left ventricular dysfunction due to myocardial infarction as a result of a coronary artery dissection [2,3,4].
Neurogenic shock can simply be caused by spinal cord ischaemia or infarction and should be considered when the patient has an obvious para- or tetraplegia with bradycardia and hypotension and warm peripheries.
Abdominal examination is essential to exclude other potential causes of the patients symptoms such as pancreatitis, perforated hollow viscus and ruptured abdominal aortic aneurysm.
The Aortic Dissection Detection Risk Score (ADD-RS) and D-dimer
The Diagnostic Challenge
Acute aortic dissection is a rare, yet serious cardiovascular emergency with a broad range of clinical presentations and the potential consequences of a missed diagnosis are grave. CT angiography is the most widely used means of reaching a definitive diagnosis and can diagnose the condition with a high degree of accuracy but carries the risk of radiation and contrast exposure. Consequently, both missed diagnosis, and over-investigation, are key concerns.
How to approach the low-to-moderate risk patient, where an acute aortic dissection is within the pool of differential diagnoses, can be a decision-making quandary for the ED clinician.
ADD-RS
The Aortic Dissection Detection Risk Score (ADD-RS) is a clinical risk stratification tool that can aid decision-making and workup in patients where acute aortic dissection is suspected.
| Clinical Finding | Points | |
|---|---|---|
| Any high-risk condition | – Marfan syndrome – Family history of aortic disease – Known aortic valve disease – Recent aortic manipulation – Known thoracic aortic aneurysm |
+1 point |
| Any high-risk pain feature | Chest, back, or abdominal pain described as any of the following: – Abrupt onset – Severe intensity – Ripping/tearing in nature |
+1 point |
| Any high-risk exam feature | – Evidence of perfusion deficit (pulse deficit, systolic BP differential, or focal neurological deficit in conjunction with a history of pain) – New murmur of aortic insufficiency (with any history of associated pain) – Hypotension or shock state |
+1 point |
Patients are considered low risk if the score is 0, intermediate risk if the score is 1, and high risk if the score is >1. Evidence suggests that around 95% of patients diagnosed with acute aortic dissection are identified as intermediate or high risk using this scoring tool.
D-dimer
D-dimer is typically elevated in patients with acute aortic dissection. Studies have looked at using D-dimer as a screening tool for AAD at a cut-off of 500ng/ml, where a positive D-dimer has been found to be around 96% sensitive for AAD.
A positive D-dimer is, of course, a very non-specific finding. However, a negative D-dimer could make for a useful rule-out test in low-risk patients.
ADD-RS + D-dimer
The ADvISED prospective multicentre study has looked at using the ADD-RS clinical risk stratification tool in combination with D-dimer as a novel clinical pathway for ruling out acute aortic dissection. In this study, using an ADD-RS score of ≤1 and negative D-dimer was 98.8% sensitive for the detection of acute aortic dissection.
The study authors propose the following diagnostic approach:
- For patients with ADD-RS >1, consider proceeding directly to CTA or other conclusive imaging
- For patients with ADD-RS ≤1, consider D-dimer testing. If D-dimer is <500ng/ml, consider stopping workup for aortic dissection and consider alternate diagnoses; if >500ng/ml, consider proceeding to CTA or other conclusive imaging.
Whilst this pathway has not been externally validated, the evidence from this study may be helpful to the ED clinician when it comes to making informed decisions. This kind of approach could help to avoid the need for CT in lower risk patients.
ECG
The 12 lead electrocardiogram is not as helpful as one may think in distinguishing aortic dissection from acute coronary syndrome as it is only completely normal in 30% of patients with dissection. In the IRAD series 3% of all aortic dissection patients had ST elevation myocardial infarction pattern; 15% acute ischaemic changes and 41% had non-specific ST segment and T wave changes.
If the history suggests aortic dissection, a diagnosis of acute coronary syndrome should not be made even if the ECG has obvious STEMI or NSTEMI patterns as antiplatelet treatment, heparin or thrombolysis may worsen the prognosis of the patient. It is always better to withhold these treatments when aortic dissection is considered and immediately arrange for urgent aortic imaging to clarify the diagnosis.

The image displays a 12 lead ECG
Chest Radiography
Chest X-ray is not a reliable investigation in the diagnosis of aortic dissection and should not delay definitive imaging in patients with a high degree of clinical suspicion where timely diagnosis is critical.
However, an erect chest x-ray is helpful in a more general sense in the work up of any patient presenting with acute chest pain and may provide another diagnosis for the patients symptoms e.g. spontaneous pneumothorax.
In aortic dissection, an abnormal chest x-ray is present most of the time and could provide an important clue to the diagnosis. The following radiological signs should be sought:
A widened mediastinum and other radiological signs
Mediastinal widening (see Figure 2) is usually the most common chest X-ray finding in patients with dissection. However, other radiological signs are important to elicit (see Figure 3). An abnormal aortic contour may occur in around half of patients. A soft tissue shadow peripheral to a calcified aortic annulus, which represents blood within the false lumen extending around the aortic annulus, is a subtle sign that occurs in a minority of patients.
Pleural effusion
A pleural effusion, representing a haemothorax (invariably massive) is seen in some patients. This typically occurs when the dissection process involves the descending thoracic aorta, and when rupture occurs here it is almost always into the left pleural space.

Figure 2: Mediastinal widening on the CXR

Figure 3: Other radiological features suggestive of thoracic aortic dissection

A soft tissue shadow peripheral to a calcified aortic annulus occurs in 15% of patients.

A globualr heart suggesting a large haemopericardium

Pleural effusion
Note however that normal chest radiography is common in patients with aortic dissection, so a normal CXR cannot rule out the diagnosis. CXR sensitivity for aortic dissection is generally estimated at around 60-90% in studies, though even where positive findings exist, these may be subtle and non-specific.
Transthoracic Echocardiography
Although transthoracic echocardiography (TTE) can be performed at the bedside in the resuscitation room it must not delay more definitive investigations such as CT or transoesophageal echocardiography.
TTE may help make the diagnosis of aortic dissection by identifying a free intimal flap within the aortic lumen but its sensitivity is approximately 80% for type A dissections but only 50% for type B [5]. Such imaging rarely identifies the extent of the dissection and a more definitive investigation is always required. It does however accurately detect a pericardial effusion, aortic regurgitation and the degree of aortic valvular disruption all of which provide valuable information for the surgeon. It is therefore ideally performed whilst awaiting interhospital transfer or whilst awaiting theatre in centres with Cardiothoracic surgery on site.
Transoesophageal Echocardiography
Transoesophageal echocardiography (TOE) is an ideal test because it can be performed in the resuscitation room, has a sensitivity of 90-98%; can easily delineate the extent of the dissection and can visualise the aortic root and valve (9). In the UK, this test is limited by its availability out-of-hours. It can also cause surges in blood pressure whilst instrumenting the awake patient particularly if the operator is inexperienced in its use.
CT scan of mediastinum
Aortic dissection is diagnosed on CT by identifying two distinct lumens with a visible intimal flap (see Figure 4). It can also delineate branch vessel involvement, visualise the entire aorta and has a sensitivity approaching 100%. CT will also reveal pericardial fluid (see Figure 5) which is not a direct confirmatory test for aortic dissection but will suggest this diagnosis in the right clinical context.
A distinct advantage of CT over other modalities of aortic imaging is that currently most hospitals in the UK are able to transfer these images to a regional cardiothoracic centre if required. This gives the surgeons adequate information on whether to transfer the patient and allows them to plan the type of surgery required prior to patient arrival.
The sensitivity of CT detection for AAD is not yet 100%: it may miss a dissection if there is complete thrombosis of one lumen or if there is similar opacification of both the true and false lumens; also, intramural haematoma may be missed as the findings are often subtle and only evident on pre-contrast images.
Intimal flaps

Figure 4: Aortic dissection The arrows demonstrate the intimal flaps in both the ascending aorta (anterior) and the descending aorta (posterior). TL is the true lumen as this has contrast within it whilst the darker false lumen (FL) does not.
Lumens

The image illustrates two distinct lumens at the level of the arch of the aorta.
Dissection flap

The arrow on the image demonstrates a dissection flap within the left common carotid artery as it comes off the arch of the aorta.
Peridcardial fluid
CT will also reveal pericardial fluid which is not a direct confirmatory test for aortic dissection but will suggest this diagnosis in the right clinical context. The white arrow highlights the pericardial fluid.

Figure 5: Aortic dissection with rupture into the pericardial sac The white arrow demonstrates the pericardial effusion
MRI and aortography
Although these imaging modalities can be used to detect aortic dissection they are rarely used [5]. MRI requires that these critically ill patients be placed on different monitoring which is magnet-proof and doesnt allow for quick access to the patient should they deteriorate once the scan has commenced. MRI at the moment also takes considerable time to acquire the necessary images.
Aortography is invasive and is not performed at most hospitals. It is now rarely used as non-invasive imaging can provide the required information.
It is essential that there is an agreed imaging modality for patients with suspected aortic dissection in individual hospitals and that the regional Cardiothoracic surgeons are happy to act on whatever imaging is to be used [6].
General principles
Patients with suspected dissection are often in pain and opiate analgesia is important both for comfort and to reduce the sympathetic response to pain which itself can cause progression of the dissection process.
Definitive treatment depends upon the type of dissection:
- Type A dissections require open surgery to prevent rupture into the pericardial sac.
- Type B dissections are managed medically but may require endovascular stenting if the patient has persistent pain, a rapidly expanding aortic diameter, or malperfusion of branch vessel organs.
It is important that patients with a type B dissection are still managed in a High Dependency Unit and referred to a vascular interventional team if complications arise [7,8].
Control of blood pressure
It is vital that patients with suspected or proven dissection should have their blood pressure actively monitored and, if necessary, controlled. Hypertension is the major problem since this increases the risk of propagation of the dissection. A lower systolic blood pressure reduces the shear stress on the aortic flap and reduces the risk of further damage. However, hypotension could increase risk of organ compromise.
In theory, we would like the systolic blood pressure to be the lowest it can be, whilst still maintaining adequate end organ perfusion. In clinical practice, a cut off target for systolic blood pressure of <120 mmHg is generally used.
Similarly, heart rate control is also important since a higher heart rate increases the frequency of maximum stress exerted on the dissection. In practice, the target HR should be at least <80 bpm, though some publications advocate the more restrictive target of around 60 bpm.
During monitoring of BP, it is important to bear in mind that in type A dissection, blood pressures in each arm may be unequal. Both arms should be monitored, at least intermittently, and therapy should be targeted at the higher reading obtained. An arterial line must be placed to facilitate accurate measurement and control of BP.
Remember that the first step to controlling BP is often to provide adequate pain control, thereby reducing sympathetic stimulus. Opiate analgesia is normally indicated.
An intravenous β-blocker is generally the optimal first line anti-hypertensive. Historically, labetalol was considered the ideal agent to be used in this setting [9]. Labetalol’s advantage is that it has mixed alpha and beta blockade activity, but it is disadvantaged by its relatively long half-life of around 3-5 hours. This could cause difficulties if bleeding occurs, or there is haemodynamic instability. Where labetolol is used, it should be given as an initial bolus and then as an infusion with invasive arterial monitoring used to guide the actual dose.
More recently, esmolol has been considered the treatment of choice due to its rapid onset and offset time, which is advantageous in the management of a potentially unstable patient. Esmolol is a cardio-selective β1 receptor antagonist. It has an onset of action within 60 seconds, reaches a steady state within 2 minutes, and has a 9-minute half-life with rapid renal clearance.
If there is a strong contra-indication to β-blockers, then non-dihydropyridine calcium channel blockers (eg. diltiazem or verapamil) could be considered, though this is rarely justified. In all cases, it may be worth involving other specialist teams (eg. intensivists) to assist with management of BP.
An important point to remember is that anti-hypertensives which predominantly work by reducing systemic vascular resistance (vasodilators) will likely cause a reflex increase in contractility of the left ventricle which will potentially worsen the dissection. This is why β-blockers are favoured in the first instance, to first lower the heart rate.
Once the HR is around 60 bpm, if the BP is still not adequately controlled then a second agent, typically a nitrate-based vasodilator, should be considered.
The characteristics of the drugs used to manage hypertension in AAD (either singly or in conjunction) are shown below.
α and β-blocker
|
Drug |
Dose |
Contraindications |
|---|---|---|
|
Labetalol |
0.25 mg/kg (usually 20 mg) as a bolus over 2 min. Further boluses of 20-80 mg are usually required every 10 min once BP controlled a continuous infusion at 2 mg/min. | Cardiogenic shock, AV block, bradycardia, COPD (relative contraindication) |
β-blockers
|
Drug |
Dose |
Contraindications |
|---|---|---|
|
Esmolol |
250-500 mcg/kg/min loading dose administered over 1 min, followed by maintenance infusion 10-50 mcg/kg/min for 4 min. Repeat loading dose and increase maintenance dose for 4 min if BP remains elevated. |
Cardiogenic shock, AV block and bradycardia |
|
Metoprolol |
Starting dose is normally 5mg injected at a rate of 1-2 mg/min. Repeat doses can be given after 5 min intervals to a total dose of 10-15 mg. | As above |
Vasodilators (second line agent – should already be on a beta blocker)
|
Drug |
Dose |
Contraindications |
|---|---|---|
|
Glyceryl trinitrate |
2-10 mg/hour infusion – titrate to blood pressure |
Hypotension, hypovolaemia HOCM, aortic stenosis |
|
Sodium nitroprusside |
0.5-1.5 mcg/kg/min infusion – titrate to blood pressure. | Severe vitamin B12 deficiency, hypotension, hypovolaemia. Beware cyanide toxicity as a side-effect – hyperventilation arrhythmias, severe metabolic acidosis. |
Non-dihydropyridine calcium channel blockers (rarely used – only where β-blockers contraindicated)
|
Drug |
Dose |
Contraindications |
|---|---|---|
|
Verapamil |
Usually 2.5-5mg over 2 minutes initially. A repeat dose can be considered after 15-30 minutes. Total maximum dose is 20-30mg. |
Broad complex tachycardias, 2nd/3rd degree AV block, severe heart failure, sick sinus syndrome, HOCM, Hypotension or shock. |
|
Diltiazem |
0.25mg/kg bolus over 2 minutes (10-20mg is often used initially) followed by continuous IV infusion at 5-15mg/hour. | As above |
Management of haemopericardium in patients with AAD
In patients with haemopericardium it is imperative that pericardiocentesis is not performed as a number of case series have demonstrated that rapid decompression of the pericardium can restart fresh bleeding with rapidly fatal consequences [10].
It is thought that the pressure gradient between the false lumen and the pericardial sac is suddenly increased when pericardiocentesis is performed thereby causing sudden and catastrophic bleeding into the pericardial sac.
As a result of this case series and several case reports also highlighting this problem, the Recommendations of the Task Force on Aortic Dissection also discourage pericardiocentesis in this context [11].
Definitive treatment
Type A
Patients with a type A dissection require urgent transfer for cardiothoracic surgery: many patients die whilst waiting especially when an inter-hospital transfer is necessary.
Urgent surgery is required for type A dissections because they have the potential to rupture into the pericardium with rapidly fatal consequences. Once a patient with a Type A dissection survives to operation the subsequent in-patient mortality after surgery is 26% [1].

Type B
Patients with a type B dissection for whom open surgery is not indicated must be assessed for the presence of complications of the dissection process. These are:
- persistent intractable pain
- a rapidly expanding aortic diameter
- development of a periaortic or mediastinal haematoma
- malperfusion of a branch vessel organs
- malperfusion due to aortic lumen compression
A meta-analysis of endovascular stent-graft placements for type B AAD showed that the procedure was successful in 95% of the patients selected for such treatment [7].
Depending upon the aetiology of the branch vessel occlusion either a stent placed in the origin of the vessel or percutaneous balloon fenestration can be used to alleviate pain or other complications.

- Aortic tears occur most commonly in the ascending aorta; subsequent haemopericardium is the leading cause of death from AAD.
- The aorta may dissect along its entire length in only a few seconds and the patient may be subsequently aymptomatic at the time of presentation to hospital.
- An abrupt or sudden onset of thoracic pain occurs in 85% of patients with aortic dissection.
- The presence of an aortic diastolic murmur in the dyspnoeic patient must always alert the physician to the possibility of aortic dissection.
- Pulse deficits, including a significant difference in BP in both arms, only occurs in 20% of patients.
- The 12 lead ECG is only completely normal in 30% of patients with more than 40% having ST segment or T wave changes.
- Patients with proven or suspected aortic dissection who have a pericardial effusion must not have pericardiocentesis performed even if cardiac tamponade is present as this procedure may cause sudden death n this context (Grade C).
- Hypertension in suspected or proven aortic dissection must be aggressively treated with a suitable intravenous agent (eg. esmolol, labetolol) using invasive arterial monitoring to reduce the progression of the dissection process (Grade D). The use of only a vasodilator can accentuate the dissection.
- Patients with a Type B dissection with complications should be considered for endovascular intervention (Grade B).
- Patients with Type A dissections for whom surgery is considered appropriate must be transferred urgently.
- There should be an agreement in place between individual hospitals and the regional Cardiothoracic centre on which imaging modality is most appropriate to avoid unnecessary delays.
- Pain is not adequately treated for fear that intravenous opiates may accentuate hypotension
- The unwary may change their initial diagnosis of aortic dissection because of a lack of supporting physical signs, a normal mediastinum on CXR or ischaemic changes on the ECG and as a consequence miss the diagnosis altogether.
- Insufficient time given to obtaining the history, which is pivotal in making the diagnosis.
- Belief that a normal transthoracic echocardiogram excludes the diagnosis.
- Lowering the threshold for making the diagnosis of aortic dissection because there is no significant difference in the blood pressures between the arms.
- Allowing the blood pressure to remain high whilst awaiting tests/transfer or treating them with the wrong drugs (e.g. a vasodilator as a single agent).
- Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000 Feb 16;283(7):897-903.
- Ohara Y, Hiasa Y, Hosokawa S. Successful treatment in a case of acute aortic dissection complicated with acute myocardial infarction due to occlusion of the left main coronary artery. J Invasive Cardiol. 2003 Nov;15(11):660-2.
- Horszczaruk GJ, Roik MF, Kochman J, et al. Aortic dissection involving ostium of right coronary artery as the reason of myocardial infarction. Eur Heart J. 2006 Mar;27(5):518.
- Cardozo C, Riadh R, Mazem M. Acute myocardial infarction due to left main stem compression: aortic dissection treated by direct stenting. J Invas Cardiol 2004;16:89-91.
- Cigarroa JE, Isselbacher EM, DeSanctis RW, Eagle KA. Diagnostic imaging in the evaluation of suspected aortic dissection. Old standards and new directions. N Engl J Med. 1993 Jan 7;328(1):35-43.
- Anand R, Cumberbatch G, Swallow R, Loehry J. Difficulties in the diagnosis of acute aortic dissection. Hosp Med 2003;64(4):241-43.
- Eggebrecht H, Nienaber CA, Neuhäuser M, et al. Endovascular stent-graft placement in aortic dissection: a meta-analysis. Eur Heart J. 2006 Feb;27(4):489-98.
- Tsai TT, Fattori R, Trimarchi S, et al. Long-term survival in patients presenting with type B acute aortic dissection: insights from the International Registry of Acute Aortic Dissection. Circulation. 2006 Nov 21;114(21):2226-31.
- Grubb BP, Sirio C, Zelis R. Intravenous labetalol in acute aortic dissection. JAMA. 1987 Jul 3;258(1):78-9.
- Isselbacher EM, Cigarroa JE, Eagle KA. Cardiac tamponade complicating proximal aortic dissection: is pericardiocentesis harmful? Circulation 1994;90:2375-2378.
- Erbel R, Alfonso F, Boileau C. Diagnosis and management of aortic dissection. Eur Heart J. 2001 Sep;22(18):1642-81.
- Sarasin FP, Louis-Simonet M, Gaspoz JM, Junod AF. Detecting acute thoracic aortic dissection in the emergency department: time constraints and choice of the optimal diagnostic test. Ann Emerg Med. 1996 Sep;28(3):278-88.
- Krenz JR, O’Brien ME, Lee J, Hayes BD. Evaluation of esmolol for heart rate control in patients with acute aortic dissection. Am J Emerg Med. 2021 Jun;44:312-314
- Rogers AM, Hermann LK, Booher AM, Nienaber CA, Williams DM, et al; IRAD Investigators. Sensitivity of the aortic dissection detection risk score, a novel guideline-based tool for identification of acute aortic dissection at initial presentation: results from the international registry of acute aortic dissection. Circulation. 2011 May 24;123(20):2213-8.
- Nazerian P, Mueller C, Soeiro AM, Leidel BA, Salvadeo SAT, et al. Diagnostic Accuracy of the Aortic Dissection Detection Risk Score Plus D-Dimer for Acute Aortic Syndromes: The ADvISED Prospective Multicenter Study. Circulation. 2018 Jan 16;137(3):250-258.
- Suzuki T, Distante A, Zizza A, Trimarchi S, Villani M, et al; IRAD-Bio Investigators. Diagnosis of acute aortic dissection by D-dimer: the International Registry of Acute Aortic Dissection Substudy on Biomarkers (IRAD-Bio) experience. Circulation. 2009 May 26;119(20):2702-7.
- Baliga RR, Nienaber CA, Bossone E, Oh JK, Isselbacher EM, et al. The role of imaging in aortic dissection and related syndromes. JACC Cardiovasc Imaging. 2014 Apr;7(4):406-24.
- von Kodolitsch Y, Nienaber CA, Dieckmann C, Schwartz AG, et al. Chest radiography for the diagnosis of acute aortic syndrome. Am J Med. 2004 Jan 15;116(2):73-7.
- Levy D, Goyal A, Grigorova Y, Farci F, Le JK. Aortic Dissection. [Updated Apr 2023]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Jan 2023.
- Evangelista A, Isselbacher EM, Bossone E, Gleason TG, Eusanio MD, et al; IRAD Investigators. Insights From the International Registry of Acute Aortic Dissection: A 20-Year Experience of Collaborative Clinical Research. Circulation. 2018 Apr 24;137(17):1846-1860.
- Isselbacher EM, Preventza O, Hamilton Black J 3rd, Augoustides JG, Beck AW, et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Dec 13;146(24):e334-e482.
- O’Connor B, Luntley JB. Acute dissection of the thoracic aorta. Esmolol is safer than and as effective as labetalol. BMJ. 1995 Apr 1;310(6983):875.

Aortas
As I write this, it’s aortic dissection awareness day. Not another blog on AAD I hear you cry…But we thought you might all like an update and a consolidation on what is happening in the world of this black swan diagnosis.

Non-traumatic Subarachnoid Haemorrhage
This session describes the management of presentations of non-traumatic subarachnoid haemorrhage in the ED.

Aortic Dissection
About 1 year ago, Pam, a 62-year-old, recently retired teacher, fit, well & active, suffered sudden onset of severe ‘ripping’ pain in her chest & upper abdomen
26 Comments
Good concise review
Good review
interesting to know pitfalls
excellent
Excellent review for revision.
helpful images!
Very hot topic
good review
Excellent, concise revision, Especially Safety Pearls and Pitfalls
Very useful
Informative
Thorough and comprehensive learning thank you
Have seen a few and the largest one was painless but STEMI changes on ECG, was about to send for PCI but X-ray showed widened mediastinum so went for CT Aorta instead!
Nice and helpfull
Succinct!
Good reading very helpful. Read it before but good to refresh my memory. Thankyou
Thanks RCEM Learning
very nicely written
Good Concise review of the topic.
Absolutely fantastic stuff.
Good review.
Very nice summary
Good teaching
great
Great learning
Very good module. Concise information.