
Author: Balaji Dorani / Editors: John P Sloan, Kathryn Louise Mahony / Reviewer: Eugene Henry, Rafeeq Ahmed Sulaiman / Code: SLO4, TC2, TC5, TP7 / Published: 02/10/2023
Soft-tissue hand injuries are a common presentation in UK emergency departments (EDs). The vast majority of such injuries have been traditionally managed by ED specialists, with only about 10-15% of patients referred to specialist centres.
This session presents a logical approach to the assessment, diagnosis and management of soft-tissue hand injuries in the ED, including suggested indications for early hand specialist referrals.
Context
- Hand injuries account for 5-10% of attendances to EDs in the UK, however 20-30% of hand injuries are improperly diagnosed and go unrecognised.
- Distinguishing an occult tendon, ligament or nerve injury from an uncomplicated laceration or crush injury requires a good understanding of hand anatomy and function, in addition to establishing accurate injury history and carrying out a thorough clinical examination.
- Optimal management of soft-tissue hand injuries in the ED will identify those patients who can be safely managed by ED clinicians, and will also ensure that those patients needing hand specialist clinic care will be identified and referred with minimal delay.
- This session discusses the presentation of common soft-tissue hand injuries, their clinical evaluation and their subsequent management, including when to make a referral to a specialist hand surgeon.
Evaluation
Hand injury evaluation follows a step-wise process of listen, look, feel and stress.

Fig.1
Important considerations are:
- Mechanism of injury
- Degree and duration of any crushing force
- Whether there is any break in the overlying skin or penetrating injury.
Use of diagrams and clear documentation are valuable.
The key points in the history when evaluating a hand injury are:
- Age
- Hand dominance
- Occupation/hobbies
- Where, when and how did the injury occur?
- What was the position of the hand at the time of injury? Injuries with the digits in flexion can result in retraction of the cut end of the tendon when the hand adopts the neutral position
Compare both hands to better assess baseline function.
Evaluation Process

Assess
Assess for any external abnormalities such as deformity, open wounds, bruising and swelling, which may indicate the nature of the injury. Pallor or cyanosis of a digit suggests vascular compromise.
Observe
Observe the posture of the hand at rest, as with flexor tendons intact the fingers assume a partially flexed position at rest, with a cascade of increasing flexion from index through to the little fingers in the image.
Loss of cascade
Loss of cascade may indicate a flexor tendon injury. In small children, uncooperative or obtunded patients, squeezing the forearm muscles while observing the fingers can also be used to assess tendon continuity.
The status
The status of hand tendons can also be assessed by passively flexing and extending the wrist. With intact extensors, passive wrist flexion causes finger extension. When flexor tendons are intact wrist extension leads to flexion of the fingers.
Recognition of Soft-tissue Hand Injuries
With regards to recognising soft-tissue hand injuries the clinician needs to be aware of:
Tendon rupture

Tendon rupture may occur without overlying skin laceration.
Tendons may rupture internally due to the following:
- The sharp bone edges at a fracture site
- Vascular insufficiency e.g. extensor pollicis longus in distal radius fracture
- Closed avulsion e.g. mallet finger
- Closed rupture e.g. central slip injury of the proximal interphalangeal joint (PIPJ)
Nerve injury

Nerve injury is an important consideration in all hand injuries.
Sensory loss following a proximal crush injury or closed fracture suggests ongoing nerve compression and may require surgical decompression.
Sensory loss in relation to a hand laceration is a sign of nerve division and requires surgical exploration.
Temporary nerve malfunction may occur in a closed injury due to mechanical trauma (neuropraxia). Serial examinations by the same observer may be useful in distinguishing neuropraxia from progressive compression neuropathy in the hand.
Two-point discrimination is the most reliable test for sensory examination of the hand [2-3]. A paper clip is usually adequate to perform this test. It can be performed as either a static or a dynamic examination. The patient should be asked to close or avert their eyes to remove any visual compensation.
The static two-point discrimination test is performed using progressively narrowing prongs from a starting point of 8 mm.
In the moving examination the prongs are moved progressively proximally to distally – across the finger being examined.
Two-point discrimination of greater than 6 mm static or 4 mm moving is abnormal [2-3].
Normal skin is slightly moist. The absence of sweating in the skin of the hand or fingers is a sign of nerve injury due to loss of sympathetic innervation. The body of a pen glides smoothly across such dry skin but not across slightly moist normal skin (pen test) [4].
Open hand injuries

In open hand injuries when the deep fascia or palmar aponeurosis are breached, clinical examination alone is unreliable, as it cannot exclude the presence of non-radio-opaque foreign bodies, or partial injuries of tendons or nerves. (Fig 3)
Adjuncts like radiographs and examination under anaesthesia may be helpful. In these circumstances, evaluation of the hand may include formal surgical exploration with tourniquet control to exclude or treat the underlying injury, wound closure, followed by early rehabilitation. Such injuries are best managed under the care of a specialist hand surgeon.
Finger Flexion
Movements of the digits are brought about by the intrinsic muscles of the hand, the tendons of the forearm flexors and the tendons of the forearm extensors.

There are two long flexors to each finger:
- Flexor digitorum profundus (FDP) inserts into the base of the distal phalanx and flexes the distal interphalangeal joint (DIPJ)
- Flexor digitorum superficialis (FDS) inserts into the sides of the middle phalanx and flexes the proximal interphalangeal joint (PIPJ)
Nerves

The ulnar nerve supplies the FDP tendons to the little and ring fingers; the other FDP tendons are supplied by the median nerve. The ulnar nerve supplies sensation over the ulnar side of the hand and little finger. It also supplies the dorsal ulnar region of the hand via the dorsal cutaneous branch of the ulnar nerve.
The median nerve supplies sensation over the palmar index, middle fingers, thumb, and proximal palm near the thenar eminence. Motor function can be tested by abductor pollicis brevis action test thumb abduction with palm up, raising the thumb to perpendicular.
Weakness or absence of flexion of the IPJ of the thumb (FPL) and the DIPJ of the index finger (FDP) against resistance, if present, are due to a more proximal lesion (anterior interosseous nerve).
Tendons (FDS and FDP)

The FDS and the FDP tendons travel distally from the forearm through the carpal tunnel, after which they traverse a fibro-osseous tunnel in each digit to insert in the respective phalanges.
The profundus tendon pierces that of the superficialis over the proximal phalanx.
The metacarpal heads, phalanges and intervening joints form the dorsal wall, with the anterolateral wall comprising of the annular pulley system and fibrous flexor sheath (condensed deep fascia attached to the margins of the phalanx).
The fibrous sheaths are lined by the synovial membrane, which reflects around each tendon.
Tendons (synovial sheaths)

The tendons of the index, middle and ring fingers have synovial sheaths that extend from the level of the FDP insertion, closing off proximally at the mid palm level at the metacarpal head.
However, the synovial sheaths of the thumb and little finger extend proximally into the palm as the radial and ulnar bursae respectively. These extend below the flexor retinaculum and communicate in about 50% of patients [5]. While more proximally, the radial and ulnar bursae are contiguous with a potential deep space (space of Perona) lying between the pronator quadratus and the FDP tendons, where an abscess may occur in hand infections.
Pulleys

The annular and cruciform pulleys form an intricate constraining sheath to keep the tendons close to the bone, preventing bowstringing when flexing the metacarpophalangeal (MCP), proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints.
Three cruciform pulleys (C1-C3) and five annular pulleys (A1-A5) exist. From a biomechanical advantage point the A2 and A4 pulleys are considered the most important to prevent bowstringing.

Finger Tendon Injury Zones
A distal-to-proximal 5-zone (I-V) classification system has been developed based on location, treatment considerations and prognosis [6]. The thumb flexor tendon injury zones differ from the fingers as the thumb has one less phalanx.
I
Zone I contains only the FDP tendon and extends from the insertion of the FDP to the insertion of the FDS tendon.
II
Zone II is the area extending from the insertion of the FDS tendon to the distal palmar crease (proximal end of the A1 pulley). This area is also known as ‘No-Man’s land’, due to the shared flexor sheath and a higher risk of adhesions.
III
Zone III is the palm area from the distal palmar crease (proximal end of the A1 pulley) to the distal border of the transverse carpal ligament.
IV
Zone IV is within the carpal tunnel.
V
Zone V is proximal to the carpal tunnel in the distal forearm.
TI
Zone TI is from the insertion of the flexor pollicis longus (FPL) to the proximal part of the A2 pulley.
TII
Zone TII is from the proximal part of the A2 pulley to the distal part of the A1 pulley.
TIII
Zone TIII is proximal to the A1 pulley as far as the carpal tunnel.

Finger Extension
Extension of the digits is a combination of extrinsic and intrinsic muscle action. The extrinsic extensors are primarily responsible for MCPJ extension, and the intrinsic extensors are primarily responsible for IPJ extension.
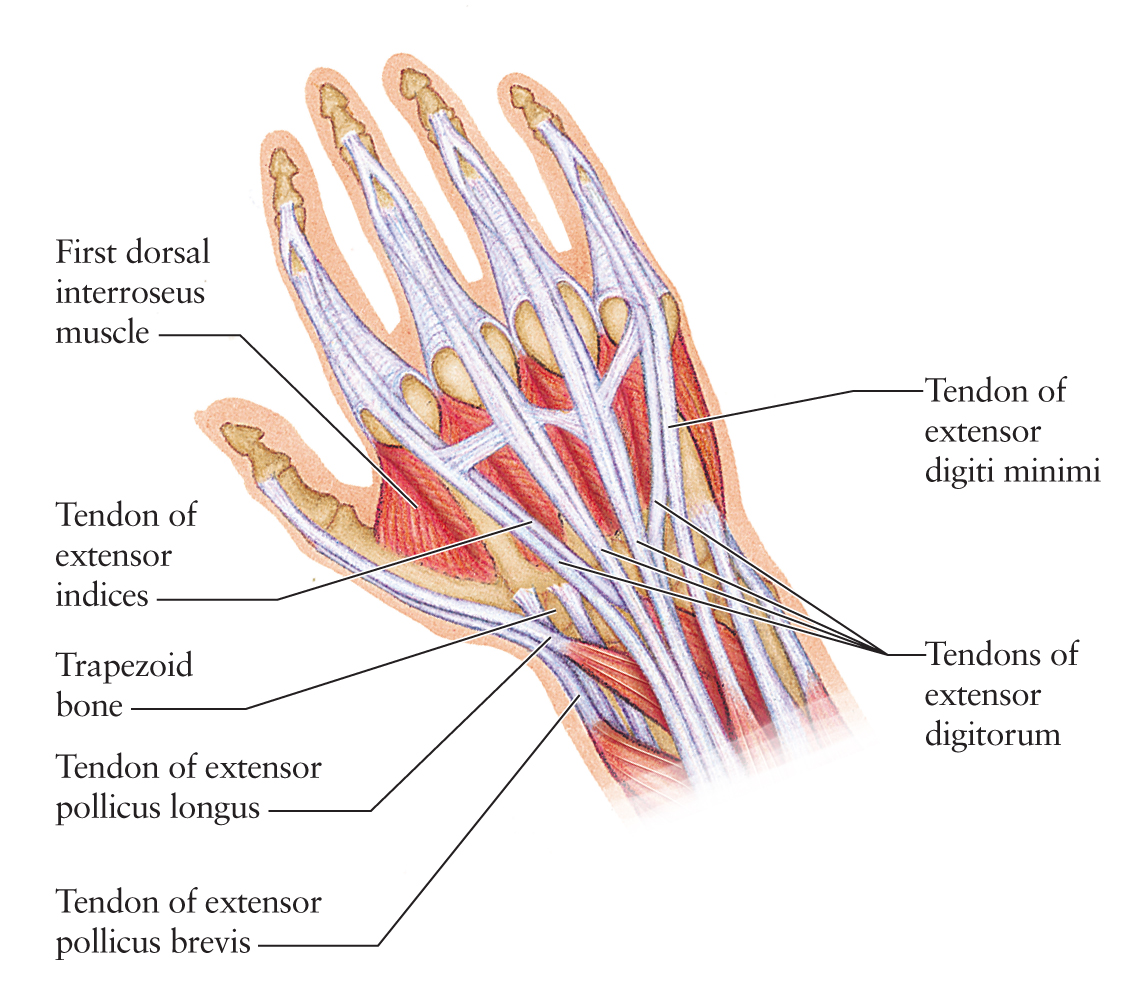
The long (extrinsic) extensors of the fingers are the extensor digitorum communis (EDC), reinforced by the extensor indicis and the extensor digiti minimi, joining the appropriate tendons of EDC on the ulnar side.
As the tendons pass over the MCP joints they are stabilised by tough transverse fibres called sagittal bands.
The tendons of the EDC terminate in each finger as an aponeurotic extensor expansion, covering the dorsum of the proximal phalanx and the side of its base. It attaches by a central slip into the base of each middle phalanx, and by two lateral slips to the base of each distal phalanx.
Extensor Tendon Injury Zones
Extensor tendon injuries are classified into eight zones [6].
Zone I is the area over the DIP joint and distal phalanx. Disruption of the tendon will cause mallet finger. The long-term consequence of this injury can be a swan-neck deformity.
Zone II is over the middle phalanx; assessment and treatment are the same as for zone I injuries.
Zone III is over the PIP joint. Injury here can result in a boutonnire’s deformity, which is hyperextension at the MCP and DIP joints.
Zone IV injuries are located on the proximal phalanx and are treated like zone III injuries.
Zone V injuries occur over the MCP joint.
Zone VI injuries are on the dorsum of the hand. The tendons are very superficial here and can be easily damaged.
Zone VII injuries involve the wrist and multiple tendons; these should be evaluated by a hand surgeon.
VIII
Zone VIII injuries are in the distal forearm. Injuries in this location often require tendon retrieval for complete lacerations and may need to be performed in the operating room.

Learning Bite
– The little finger FDS is absent in approximately 20% of individuals
– Extensor zones can easily be recalled by remembering that the odd numbers overlie the joints
– The thumb has no zone III since there is only one interphalangeal (IP) joint.
Finger Anatomy
The margins of the extensor expansion over the dorsal aspect of the proximal phalanges and PIPJs are reinforced by tendons of the intrinsic muscles of the fingers.
The dorsal and palmar interossei arise from the sides and fronts of the metacarpals respectively.
The lumbricals are distinctive as they take origin from (and are inserted into) tendons; they arise from the four profundus tendons and run on the radial side of the MCPJ to join the extensor expansion.
The palmar intrinsic muscles all flex the MCPJ and extend the IPJ. In addition, the three palmar interossei adduct the fingers (relative to the middle finger), and the four dorsal interossei abduct the fingers.
The little finger is assisted by the abductor digiti minimi (ADM) in abduction. The ADM, together with the opponens digiti minimi and the flexor digiti minimi, form the hypothenar eminence.
Examination
When examining the flexor and extensor tendons of the hand, the inspection should take into consideration:
- Hand position – look for the normal cascade
- Symmetry
- Deformities
- Swelling, colour, wounds (fig 1), wasting, scars
What is the aim of palpation?
Palpation should:
- Localise tenderness: bony and soft tissue
- Define the characteristics of the swelling
What should be examined in terms of range of motion?
Active and passive range of motion should be examined, and the range of motion against manual resistance to strength:
- Finger flexion at MCP, PIP, DIP joints
- Finger extension at MCP, PIP, and DIP joints
- Finger abduction
- Finger adduction
- Thumb flexion
- Thumb extension
- Thumb abduction
- Thumb adduction
- Opposition of thumb to little finger
- Functional grip tests
- Pinch tests
What neurovascular examinations should be undertaken?
Neurovascular examinations should include:
- Regional pulses, capillary refill
- Test sensation
What special tests are there?
Special tests include:
- FDS, FDP, FPL, EPL testing
- Extensor tendon testing for mallet finger
- Elson’s test
- Ligamentous instability test of the thumb
When should you x-ray?
X-ray when a fracture, a penetration injury, or a foreign body are suspected.

Nerve Injury

Nerve injuries may occur as a result of blunt, penetrating or crush injuries.
Median nerve
The median nerve motor and sensory function should be tested as follows:
- Thumb abduction with the palm up, raising the thumb to perpendicular (AbPB)
- Sensation over the palmar index finger, thumb, and proximal palm near the thenar eminence
- Weakness or absence of flexion of the IPJ of the thumb (FPL) and the DIPJ of the index finger (FDP) against resistance, if present, are due to a proximal lesion (anterior interosseous nerve).
Ulnar nerve
The ulnar nerve motor and sensory function should be tested as follows:
- Spread the fingers against resistance (dorsal interossei)
- Adduct the fingers against resistance (palmar interossei)
- Thumb adduction (AdP) against the index finger, and with paper interposed and pulled away (Froments sign look for use of FPL, supplied by the median nerve, to assist adduction)
- Sensation over ulnar side of the hand and little finger. It also supplies the dorsal ulnar region of the hand via the dorsal cutaneous branch of the ulnar nerve
Radial nerve
The radial nerve motor and sensory function should be tested as follows:
- Finger and wrist extension
- Sensation to the dorsal first web space of the hand
Sensation
Sensation is best tested with two-point discrimination [7]. Two-point discrimination greater than 6 mm static or 4 mm moving is abnormal [2-3]. Injured and non-injured fingers should be compared. A paper clip provides an accessible testing tool [8].
As patients may guess correctly by chance, the test should be repeated at least 2-4 times on each side of the digit. Less than 80% accuracy or indeterminate testing suggests the possibility of digital nerve injury [9].
A sensory nerve deficit also implies a possible digital arterial injury given the close proximity of the two structures.
Dry, shiny skin
Nerve injury is also suggested by dry, shiny skin that does not wrinkle when immersed in water [10] this is due to a loss of sympathetic innervation.
The tactile adherence test [11] can also prove useful, looking for a loss of friction in the denervated area due to absent sweating.
It should be noted that all the above tests are subjective.
Early recognition
The early recognition of nerve injury is important as primary repair has been found to be superior to delayed repair [12].
Results of digital nerve repair are variable; in a review of 109 cases, no patients regained normal sensation, although 83% did achieve sensory results that could be classed as good [13].
Results are better in children than in adults [14].
Tendon Evaluation Tests
The specific tests required for tendon evaluation include:
Flexor digitorum superficialis (FDS)

Testing the flexor digitorum superficialis (FDS):
The patient should bend the finger whilst the others are held in full extension (thereby inactivating the deep flexors). The DIPJ should be flaccid. The exception is the index finger, which has a separate muscle belly so that extending the other digits does not isolate the FDS. For FDS to the index finger test by checking the resisted PIPJ flexion while keeping the DIPJ extended.
Flexor digitorum profundus (FDP)

Testing the flexor digitorum profundus (FDP):
With the examiner holding the PIPJ in extension, the patient should be asked to flex the tip of the finger.
Extensor tendons

Testing the extensor tendons
The fingers should be straightened against resistance. The long extensors straighten at the MCPJ, and resistance should be applied to the dorsum of the proximal phalanx. Extension at the PIPJ can be caused by the intrinsic muscles. Observe for loss of active extension at the DIPJ, i.e. a mallet deformity.
Flexor pollicis longus (FPL)

Testing the flexor pollicis longus (FPL)
Hold the thumb over the proximal phalanx and ask the patient to bend the tip.
Extensor pollicis longus (EPL)

Testing the extensor pollicis longus (EPL)
With the patient’s hand palm-down on a table, ask the patient to lift up his/her thumb, against resistance.
Management

The image shows FDP and FDS rupture due to glass injury in Zone II of the little finger. Management of flexor tendon injuries involves the following:
Asessment
In assessing tendon function, the full range of motion of each tendon against resistance should be assessed.
Up to 90% of a tendon can be lacerated with preservation of the range of active motion without resistance.
Treatment
Early surgical treatment of flexor tendon lacerations, followed by a postoperative passive-motion rehabilitation programme [15], are necessary to achieve satisfactory outcomes.
Learning Bite
Partially lacerated flexor tendons – physiologic loads may be tolerated by a tendon that has a partial laceration involving up to 75% of the cross-sectional area. Although an unreliable sign, suspect it if there is pain on resisted flexion.
Wounds
Open hand wounds, due to sharp or penetrating objects, such as glass, need careful clinical evaluation. ED assessment must include clinical examination of tendon, nerve and vascular function.
Furthermore, all penetrating wounds that breach the deep fascia or palmar aponeurosis need to be identified. Such injuries require formal surgical exploration with suitable anaesthesia and tourniquet control because clinical examination alone will not confidently exclude significant injuries to tendons, nerves or blood vessels.
Partial flexor tendon lacerations involving less than 60% of the tendon are not always repaired [15], although they should still be referred for evaluation, as they may benefit from tendon debridement and postoperative rehabilitation.
Learning Bite
In the unconscious or uncooperative patient, compression of the forearm flexor muscles can also be used to test the integrity of the flexor tendons in the hand.
As the forearm is compressed, the digits are drawn into flexion. The digits also extend and flex when passively moving the hand and wrist through flexion and extension. Neither of these tests will exclude a partial tendon injury.
Mallet Finger (Zones I and II)

Clinical presentation
Zone I and Zone II extensor tendon injuries may result in a mallet deformity, due to loss of continuity of the conjoined lateral bands at the DIP joint.
The history is usually a direct blow that forcibly flexes an extended finger. However, the trauma may also be minor, or even forgotten. If left untreated, apart from being painful, the digit becomes hooked and may eventually develop a swan-neck deformity due to compensatory hyperextension at the PIP joint.
Open injuries should be referred to a hand surgeon for primary repair.
Clinical management
Radiographs
Closed mallet finger injuries are usually treated conservatively.
Mallet finger deformity may be due to bone or soft-tissue injury and radiographs are needed to confirm this.

Referral criteria
Criteria for referral include:
- The absence of full passive extension (indicating possible bony or soft-tissue entrapment requiring surgical intervention)
- Joint subluxation or an avulsion fracture of more than one-third of the articular surface
There is evidence [16-17] to suggest that even the latter injury may be treated non-operatively with good patient satisfaction, although studies with longer follow-up are required to assess the effects of resultant DIPJ arthritis on treatment outcome.
Splinting
Conservative treatment entails continuous splinting of the DIPJ in neutral or slight hyperextension for at least six weeks.
There is insufficient evidence [18, 19] to recommend any particular splint; all achieve similar outcomes, patient compliance being the key to a successful outcome.
Learning Bite
A well-fitting splint for a mallet finger is vital to ensure compliance and avoid skin breakdown, the main complication of conservative treatment. The PIPJ must be left free to allow mobilisation and prevent stiffness.
Rupture or Division of the Central Slip

Clinical presentation
Zone III injuries may involve rupture or division of the central slip (as in the image) and if unrecognised can result in the boutonnire deformity – characterised by flexion at the PIPJ and hyperextension at the DIPJ and caused by the unopposed action of FDS and volar displacement of the lateral bands. Direct visualisation in an open laceration is the easiest way to confirm and treat this injury. A simple suture followed by six weeks splintage of the PIP joint in extension is usually satisfactory.
Closed rupture of the central slip over the PIPJ is easily missed. The history may be of axial loading or forced flexion with the PIPJ in extension, or after a volar dislocation of the PIPJ. Clinically, presentations may be variable – patients may present with an acute boutonniere deformity, with an unreduced volar dislocation or, most commonly, with a painful, swollen PIPJ.
Clinical management
Examination
Examination should look specifically for maximal localised tenderness over the dorsal aspect of the PIPJ, at the insertion of the central slip. Bruising may be noticed in the area.
Active extension at the PIPJ does not exclude a rupture as, in the acute setting, full extension may still be achieved by the lateral bands.
Elson’s test
Various clinical, non-invasive tests have been described for early diagnosis of closed central slip rupture including the test described by Elson [20].
Elson’s test is performed with the PIP joint of the injured finger flexed 90 over the edge of a table. The patient then tries to extend the PIP joint of the injured finger against resistance. The absence of extension force at the PIP joint and fixed extension at the DIP joint are signs of complete rupture of the central slip.
However, the test will not demonstrate a partial rupture, and may be limited by pain and the patient’s cooperation.
See here for a video demonstration.
Boutonnire deformity

X-ray may show an avulsion fracture, and sometimes gives the first clue to a developing boutonnire deformity.
Treatment
If a central slip rupture is known or strongly suspected, the PIPJ should be splinted in a static extension splint, leaving the DIPJ free.
Further follow-up in a hand clinic is required. The swollen, painful PIPJ with full active extension should be followed up in an ED clinic at 2-3 days for senior clinician re-assessment for possible central slip injury.
Lacerations (Zone IV)

Zone IV tendon injuries over the proximal phalanx are usually due to lacerations.
The ED management should include a wound exploration under local anaesthetic cover.
Confirmed tendon injuries need referral to a hand surgeon for tendon repair, splinting and follow-up.
Open Zone V Injuries

Clinical presentation
Open zone V injuries overlie the MCPJ. Open injuries in this area must be suspected to be a human bite until proven otherwise [3]. Indeed such injuries are called ‘fight bites’, and in addition to tendon injury, joint involvement and septic arthritis are likely.
Due to the broad sagittal band and extensor tendon interconnections, the ruptured tendon does not retract and extensor lag is usually mild. The position of the joint at the time of injury must be remembered as the tendon laceration may be proximal to the skin wound.
Clinical management
ED management of open zone V injuries may include a wound exploration to establish the depth of the wound and any tendon or joint involvement. Alternatively, these injuries may be referred urgently to a hand surgery unit.
It is recommended that all zone V wounds require surgical exploration and any joint involvement needs thorough debridement and washout. Admission for hand elevation and IV antibiotics is also required. Zone V tendon injuries from a human bite should undergo delayed repair when the risk of infection and septic arthritis are minimised [2].
Closed Zone V Injuries
Clinical presentation
Closed zone V injuries in this area may also present as a subluxation or dislocation of the extensor hood. The tendon usually subluxes in an ulnar direction, due to a tearing of the sagittal fibres on the radial side, with the middle (long) finger being the most commonly affected [21].
The injury is of forced flexion or extension at the MCPJ, with immediate pain and a persistent loss of extension of the affected finger. There may be a painful popping sensation over the dorsum of the hand with attempts at movement. Active extension of the MCPJ is weak or absent. However, once passively corrected, with the tendon having relocated centrally, the patient will be able to maintain extension actively.
Clinical management
Hand surgeon referral is required as both surgical repair and conservative management with splintage are possible.
Zone VI Injuries

Zone VI injuries frequently involve tendon damage due to their superficial site over the dorsum of the hand. When assessing extension, care is advised because, if the laceration is proximal to the junctura tendinae, the patient may be able to extend the involved MCPJ despite a ruptured tendon. Weak extensor forces are transmitted to the junctura from adjacent extensor tendons.
ED management may include a wound exploration to identify any tendon injury. Confirmed tendon injuries require surgical repair for which hand surgery referral is required.
Zone VII and VIII Injuries

Zone VII and Zone VIII injuries involve the wrist and forearm, with possible damage to the extensor retinaculum.
Open injuries to these areas require surgical exploration and should be referred to a hand surgeon.
High Pressure Injection Injury
This seemingly innocuous injury is often underestimated and underrecognized. The injury is characterized by a small puncture wound and injection of liquid (lubricants, oils, solvents etc) into the hand using high pressure guns (2000 to 12000 psi). The wounds are small, but the underlying damage is usually extensive. The injected substance leads to extensive tissue damage (local necrosis and oedema). As a result, this may lead to compartment syndrome of the affected limb. Due to their potential morbidity, injection injuries are characterized as “the most urgent of all emergencies of the hand”
These patients would require immediate referral to the Hand Surgeons for debridement. ED management includes intravenous antibiotics and tetanus prophylaxis.
Introduction

Fingertip injuries are the most common hand injuries in adults and account for approximately two-thirds of hand injuries in children. Damage to the nail bed is reported to occur in 15-24% of fingertip injuries [2].
What damage occurs with a fingertip injury?
Fractures proximal to the waist of the terminal phalanx or intra-articular fractures require specialist surgical assessment to determine the need for internal stabilisation.
How can a fingertip injury be defined?
A fingertip injury is defined as any soft tissue, nail or bony injury distal to the dorsal and volar skin creases of the distal interphalangeal joint and insertions of the long flexor tendons of the fingers or thumb.
Learning Bite
Approximately half of fingertip injuries have an associated fracture of the digit, usually the distal tuft of the terminal phalanx [3], which requires external splintage only.
Fractures proximal to the waist of the terminal phalanx or intra-articular fractures require specialist surgical assessment to determine the need for internal stabilisation.
Fingertip Anatomy
The nail plate consists of onychia, which has similar qualities to the keratin on normal skin. Proximally the nail is produced by the dorsal roof of the nail fold, the germinal matrix [2-3].
Distally the nail plate rests on the sterile matrix to which it is intimately attached through the longitudinal nail furrows and ridges. Proximally the nail plate is enclosed by the eponychium and on the sides by the perionychium and distally by the hyponychium. The lunula is a visible white area of the proximal nail bed distal to the eponychium and represents the transition from germinal matrix to sterile matrix. The distal phalanx supports the nail plate and if the bone is too short due to trauma, it will lead to loss of support and a hook nail type of deformity.

The fingernail and its underlying matrix are supported by more than half the bone length of the underlying terminal phalanx. In the distal pulp of the finger the skin is stabilised by fascial bands running from skin to bone, which contain loculated fat; this arrangement stabilises the fingertip pulp skin under pressure. Nail growth is slow, approximately 0.1 mm daily [2], but often with an initial delay following traumatic avulsion, hence may take 4-6 months to grow back fully and up to 12 months to achieve maturity.
Fingertip Amputations

The fingertip is the part of the terminal phalanx that is distal to the insertion of extensor and flexor tendons. Fingertip injuries can be the result of crushing, tearing (lacerating) or tissue loss (amputating injuries).
Learning Bite
Fractures proximal to the waist of the terminal phalanx, or intra-articular fractures in fingertip injuries, require specialist surgical assessment to determine the need for internal stabilisation.
Transverse amputations
Partial amputations are commonly seen in crush injuries. Children may get fingertips crushed in doors or furniture.
Fingertip injuries with tissue loss can be classified by the residual defect.
Transverse amputations are classified as shown in the table and image.
| Type I | Fingertip soft-tissue loss only |
| Type II | Fingertip loss at the level of the proximal third of the nail plate |
| Type III | Fingertip loss at the level of the eponychial fold |
| Type IV | Fingertip loss proximal to the DIP joint |

Oblique fingertip defects

Oblique fingertip defects can be classified in one of three ways – volar, dorsal and lateral [3].
Non-operative treatment
Emergency physician
Conservative treatment has the advantage of convenience, simplicity and low associated costs. Some fingertip injuries can be managed adequately in an emergency department under the care of an emergency physician.
The little finger of a ‘size 6’ glove makes a good finger tourniquet. A small hole is cut into the tip and the finger glove is rolled on to the finger from distal to proximal. This serves to exsanguinate the digit and provides tourniquet to the digit.
Learning Bite
It is imperative that the tourniquet is removed and finger circulation checked before occlusive dressings are applied.
ED specialist
Fingertip injuries suitable for management by an ED specialist are:
- Superficial skin loss defect <1 cm2 in Zone I
- Transverse Type I fingertip amputations
- Type I and Type II fingertip amputations in children
- Oblique partial fingertip amputation without bone exposure
- Stable fracture needing splintage only
Follow-up clinic and dressings facilities, as well as access to a physiotherapist, are required.
It is to be noted that children have greater tissue regeneration and modelling capacity.
ED procedure
The procedure for carrying out treatment of fingertip injuries in the ED is:
- Local anaesthesia ring block, essential for assessment, treatment and analgesia
- Cleanse thoroughly, remove dirt and foreign material
- Trim off any devitalised tissue
- Non-adherent dressings to be changed and the wound inspected 2-3 times weekly
- A stable fracture of the terminal phalanx may be externally splinted for 2-3 weeks
- A 1 cm2 defect takes an average of five weeks to heal [3]
Learning Bite
The fingernail and its underlying matrix are supported by more than half the bone length of the underlying terminal phalanx
Type I and Type II amputations have sufficient bone support for straight nail regrowth without hook nail deformity
Following nail bed repair the avulsed nail can be placed in the nail fold, which acts as a template and stent for the nail bed and also decreases discomfort by acting as a natural protective cover
Fingertip Amputations (Hand Specialist)

A patient would be referred to a hand specialist if he/she presented with any of the following:
- Type II or higher partial amputation of the fingertip
- Oblique fingertip partial amputation with bone exposure or fracture
- A large soft-tissue defect >1 cm2
- An unstable fracture of the terminal phalanx
Do not discard the amputated part until you have thoroughly examined the wound. It may be possible to use some of the skin from the amputated segment as a skin graft to cover the open wound.
Surgical options
Possible surgical options for a hand specialist include:
- Bone shortening and primary skin closure
- Tip reposition
- Local skin flap
- Regional skin flap
- Distant skin flap
- Skin graft
- Toe pulp transfer
- Replantation
- Micro vascular flap
Patient preparation
To prepare a patient for transfer to a hand specialist unit carry out the following procedure:
- Administer intravenous (IV) fluids if the patient needs fasting for a general anaesthetic and for patient hydration
- Give IV antibiotics. A first-generation cephalosporin is appropriate
- Control pain with IV morphine or a digital block
- Get a radiograph of the digit and also of the amputated segment (if available)
- Clean and dress the finger stump with non-adherent dressing, and wrap the stump lightly with sterile dressings and bandage
- Elevate the affected hand in a sling
- Tetanus prophylaxis
- The patient is now ready for transfer
Care of the amputated part
In order to take care of the amputated part carry out the following procedure:
- Remove any foreign material from the exposed soft tissues
- Clean the amputated part with saline, and wrap it in saline moistened gauze (damp, not soaking wet)
- Place the wrapped segment in a plastic bag
- Place the bag into a container filled with ice mixed with saline. DO NOT place the amputated part directly on ice [2]
- Ensure that the bag containing the amputated part is appropriately labelled i.e patient details and part

Sharp forceful injuries that penetrate the nail plate will usually continue through the bony phalanx and result in fingertip amputation.
However, the majority of fingertip injuries are due to crushing between two hard and blunt objects. This mechanism causes the nail plate to buckle and compress the nail plate against the terminal phalanx bone. Depending on the force of the crushing injury, the nail bed may sustain a simple or stellate laceration. A very high energy crush can shatter both the terminal phalanx bone and nail bed into many fragments.
Subungual Haematoma

Crush injuries of lesser severity may cause subungual haematoma. A small nail bed laceration with resultant bleeding occurs, which cannot drain from an intact nail. These can be excruciatingly painful. Painful subungual haematomas should be drained to relieve both pain and pressure.
It has previously been recommended that larger subungual haematomas involving 25-50% of the visible nail require nail removal for examination of the nail bed and repair, however, prospective studies comparing simple haematoma decompression versus nail plate removal and formal nail bed repair have shown no notable difference in outcome.
Small subungual haematomas can be relieved by simply decompressing through a drain hole in the nail by needle trephining using a hot paper clip or battery-powered cautery.
In the ED, if the nail plate is still adherent to the nail bed and not displaced out of the nail fold, regardless of the size of the subungual haematoma, conservative treatment is recommended. In this situation the haematoma may be drained, but the nail need not be removed for nail bed repair.
Lacerations and Avulsions

Nail bed lacerations
Nail bed lacerations should be suspected in all fingertip crush injuries. Simple or stellate nail bed lacerations without underlying fractures have a better prognosis than nail bed avulsions [3].
These injuries can be repaired by separating and removing the nail plate from the nail bed with fine scissors. The nail bed is carefully repaired with fine absorbable sutures such as Vicryl Rapide 6.0. Such repair should include the dorsal roof and ventral floor of the nail fold.
The removed nail is trimmed of sharp edges and replaced in the nail fold to act as a stent for the nail bed, a template for the new nail, and as a protective cover to reduce pain and discomfort. A transverse suture through the nail and lateral folds will help retain the nail in position.
It is our practice to retain the nail for four weeks before discarding it by cutting the retaining sutures.
Nail bed lacerations with associated fractures
The nail bed is supported internally by the terminal phalanx bone and externally by the nail plate. Nail bed lacerations associated with stable undisplaced fractures of the terminal phalanx bone, which do not require internal fixation, are best managed by simple nail bed repair, as described previously, with external splintage alone.
However, displaced or unstable fractures should be referred for specialist treatment as they will require accurate reduction and internal stabilisation, usually with Kirschner wires prior to nail bed repair. Any residual dorsal step deformity of the terminal phalanx bone can result in nail bed irregularity, scarring, nail plate detachment and late nail deformity.
Learning Bite
Specialist referral is required due to a high risk of hook nail deformity in: nail bed lacerations with an underlying displaced or unstable fracture; nail bed avulsion; type III and IV fingertip injuries.
Nail bed avulsions
Nail bed avulsions may be in the form of a distally based flap with the nail attached proximally. The matrix may be detached from the underlying bone. Free segments of nail matrix may also be avulsed but still attached to the under surface of the traumatically avulsed nail.
These injuries are best referred to a hand specialist as meticulous repair (e.g. loupe magnification, nail bed grafting or rotational flap surgery) may be required.
Injuries to the UCL of the Thumb
Acute ruptures of the ulnar collateral ligament (UCL) of the metacarpophalangeal (MCP) joint of the thumb are due to forced radial deviation of the thumb. It is estimated that the incidence of thumb UCL rupture injuries in the UK is about 50 per 100 000 new ED attendances per annum.
The terms ‘Gamekeeper’s thumb’ and ‘Skier’s thumb’ are often used interchangeably to describe injuries to the UCL [2]. However, Skier’s thumb is a more acute injury, acquired by a falling skier. Gamekeepers acquire the injury over time as the result of chronic repeated trauma sustained due to using the thumb to snap rabbits necks, resulting in repeated stretching of the UCL.
Today, most cases of ligament damage in the MCP joint are caused from sports injuries.
UCL Anatomy and Function

The UCL proper runs from the head of the thumb metacarpal bone to the volar aspect of the proximal phalanx. Its action is to tighten in flexion and relax in extension of the MCP joint.
The accessory UCL lies anterior to the UCL proper and inserts into the volar plate. This ligament tightens in MCP joint extension and relaxes in flexion.
The adductor pollicis aponeurosis inserts to the dorsal thumb tendons and capsule of the MCP joint.
Stability
The MCP joint of the thumb maintains ulnar side stability by means of both static and dynamic mechanisms. Static stability is provided by the main and accessory UCLs, the volar plate, as well as the dorsal capsule.
The adductor pollicis muscle and tendon in the first web space of the hand also provide dynamic stability, ulnar support and restraint to the MCP joint of the thumb.
Injury
Due to the anatomical arrangement in this area, UCL injuries may also involve injuries to the accessory UCL, volar plate, dorsal capsule, adductor pollicis insertion, and may also have associated fractures of the proximal phalanx.
Diagnosis and Treatment
The diagnosis and treatment of injuries to the UCL involves the following:
Examination
Examination of the injured thumb should always be preceded by examination of the normal uninjured thumb. Administration of a local anaesthetic facilitates the clinical assessment.
Normally there is some laxity in the UCL of 15 degrees (+/-5 degrees), but little variability from left side to right side. Pain, swelling, tenderness and joint stiffness localised to the ulnar side of the MCP joint are all likely to be present.
Delayed presentation may be associated with considerable pain, local swelling and tenderness, which may make clinical examination difficult. It is, however, useful to identify the point of greatest tenderness.
A palpable lump or fullness on the ulnar side of the MCP joint may represent an avulsion fracture or a Stener lesion [2].
Learning Bite
A Stener lesion is a palpable lump on the ulnar side of the MCP joint of the thumb. It signifies a ruptured and retracted UCL with its proximal stump separated from its distal stump by the interposed adductor pollicis aponeurosis.
Radiographs
Before stress testing the UCL of the thumb, it is advisable to obtain radiographs.
In the presence of a fracture, treatment can be based on the position of the thumb and displacement of the fracture, instead of stress testing [2].
Stress testing
In the absence of an associated fracture, stress testing of the ulnar stability of the thumb MCP joint can be performed in full extension (accessory UCL) and 30o flexion (UCL proper), since the UCL proper is under maximal tension in this position.
Care is needed while stress testing, since too vigorous an examination carries the risk of conversion of an undisplaced UCL rupture into a Stener lesion, or may displace a previously undisplaced fracture [2].
In patients with a partial UCL tear, the MCP joint should be either stable, or minimally lax in both flexion and extension, when the proximal phalanx is stressed radially. The presence of a distinct end point to the opening of the joint to radialward stress suggests an incomplete tear of the UCL [3].
Learning Bite
UCL laxity of over 35o in extension and over 15o in 30o MCP joint flexion, in comparison to the contralateral side on stress testing, are considered diagnostic of a complete rupture of the UCL [3].
Ultrasound
Ultrasound scanning has been shown to be of value in the diagnosis of UCL injuries of the thumb.
Ultrasound has been shown to improve the positive predictive value of clinical examination alone from 80% to 94% in a study undertaken in a British ED.
Other options include stress radiography and arthrography.
Referral to a hand clinic
Indications for referral to a hand clinic are:
- Stener lesion
- Complete rupture of the UCL
- Displaced, rotated or large fracture fragment of the base of the proximal phalanx bone
- Subluxation or instability of the MCP joint
- Ongoing uncertainty of the severity of the UCL rupture or Stener lesion
Conservative treatment
For incomplete UCL tears the authors preferred treatment is by immobilisation in a short thumb spica cast for four weeks to allow the ligament to heal. Thereafter, the cast can be discarded in favour of a short thermoplastic splint.
Supervised mobilisation is commenced at four weeks with all splints discarded after six weeks. Patients should avoid stressful activities with the injured thumb for 10-12 weeks [3].
- Quaba AA. McCarthy: Plastic Surgery. Volume 7 & 8. The Hand May and Littler W. B. Saunders, 1990. The journal of hand surgery. 1990 Apr 1;15(2):273–3. doi:10.1016/0266-7681_90_90138-T
- Martin DS, Collins ED. Manual of Acute Hand Injuries. Philadelphia: Mosby, 1998:72-73.
- Peimer CA. Surgery of the Hand and Upper Extremity, Volume 1. New York: McGraw-Hill, 1996:1045-1055.
- Harrison SH. The tactile adherence test estimating loss of sensation after nerve injury. Hand. 1974 Jun;6(2):148-9. doi: 10.1016/0072-968x(74)90079-5.
- Ellis H. Clinical Anatomy. 10th edn. Oxford: Wiley-Blackwell, 2002:217-218.
- Kleinert HE, Verdan C. Report of the Committee on Tendon Injuries (International Federation of Societies for Surgery of the Hand). J Hand Surg Am. 1983 Sep;8(5 Pt 2):794-8.
- MOBERG E. Objective methods for determining the functional value of sensibility in the hand. J Bone Joint Surg Br. 1958 Aug;40-B(3):454-76. doi: 10.1302/0301-620X.40B3.454.
- Finnell JT, Knopp R, Johnson P, Holland PC, Schubert W. A calibrated paper clip is a reliable measure of two-point discrimination. Acad Emerg Med. 2004 Jun;11(6):710-4.
- Davenport M, Tang P. Injuries to the Hand and Digits. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e. McGraw Hill; 2016. [Accessed September 13 2023].
- Vasudevan TM, van Rij AM, et al. Skin wrinkling for the assessment of sympathetic function in the limbs. Aust N Z J Surg. 2000 Jan;70(1):57-9.
- Harrison SH. The tactile adherence test estimating loss of sensation after nerve injury. Hand. 1974 Jun;6(2):148-9.
- Birch R, Raji AR. Repair of median and ulnar nerves. Primary suture is best. J Bone Joint Surg Br. 1991 Jan;73(1):154-7.
- Tupper JW, Crick JC, Matteck LR. Fascicular nerve repairs. A comparative study of epineurial and fascicular (perineurial) techniques. Orthop Clin North Am. 1988 Jan;19(1):57-69.
- Steinberg DR, Koman LA. Factors affecting the results of peripheral nerve repair. In: Gelberman RH, ed. Operative nerve repair and reconstruction. Philadelphia: JB Lippincott, 1991:349-364.
- Boyer MI, Strickland JW, et al. Flexor tendon repair and rehabilitation: state of the art in 2002. Instr Course Lect. 2003;52:137-61.
- Kalainov DM, Hoepfner PE, et al. Nonsurgical treatment of closed mallet finger fractures. J Hand Surg Am. 2005 May;30(3):580-6.
- Wehbé MA, Schneider LH. Mallet fractures. J Bone Joint Surg Am. 1984 Jun;66(5):658-69.
- Handoll HH, Vaghela MV. Interventions for treating mallet finger injuries. Cochrane Database Syst Rev. 2004;(3):CD004574.
- Maitra A, Dorani B. The conservative treatment of mallet finger with a simple splint: a case report. Arch Emerg Med. 1993 Sep;10(3):244-8.
- Elson RA. Rupture of the central slip of the extensor hood of the finger. A test for early diagnosis. J Bone Joint Surg Br. 1986 Mar;68(2):229-31.
- Inoue G, Tamura Y. Dislocation of the extensor tendons over the metacarpophalangeal joints. J Hand Surg Am. 1996 May;21(3):464-9.
- Dailiana HZ, Kotsaki D, Varitimidis S, et al. Injection injuries: seemingly minor injuries with major consequences. Hippokratia. 2008 Jan;12(1):33-6.

Common Entrapment Syndromes
Nerve entrapment syndromes are a group of conditions in which peripheral nerves are damaged, through compression or repeated trauma.

Peripheral Neuropathy
Peripheral neuropathy is a pathological process affecting a peripheral nerve or nerves (includes cranial nerves).

Elbow Injuries
Elbow injuries are common and acute elbow trauma accounts for 2-3% of all visits to the emergency department.
13 Comments
It covers all types of hand injuries with management
Excellent demonstration of both serious and mild injuries management.
Brilliant summary
All ANPs and GP Working in UTC should read it. I tell them in teaching session
good module
absolutely useful lesson..
Useful
very useful
Concise and very informative .
Consise and informative.
Great session
Excellent module for all.
Very informative, useful and easily applicable in EDs.
Excellent description and recaputulation of hand injuries.